

Sex Disparities in Applied Force on Maxillary Incisors Among Novices During Laryngoscopy Using a High-Fidelity Simulator: A Prospective Observational Study
- PMID: 38462525
- PMCID: PMC11006240
- DOI: 10.24546/0100486397
Sex Disparities in Applied Force on Maxillary Incisors Among Novices During Laryngoscopy Using a High-Fidelity Simulator: A Prospective Observational Study
Abstract
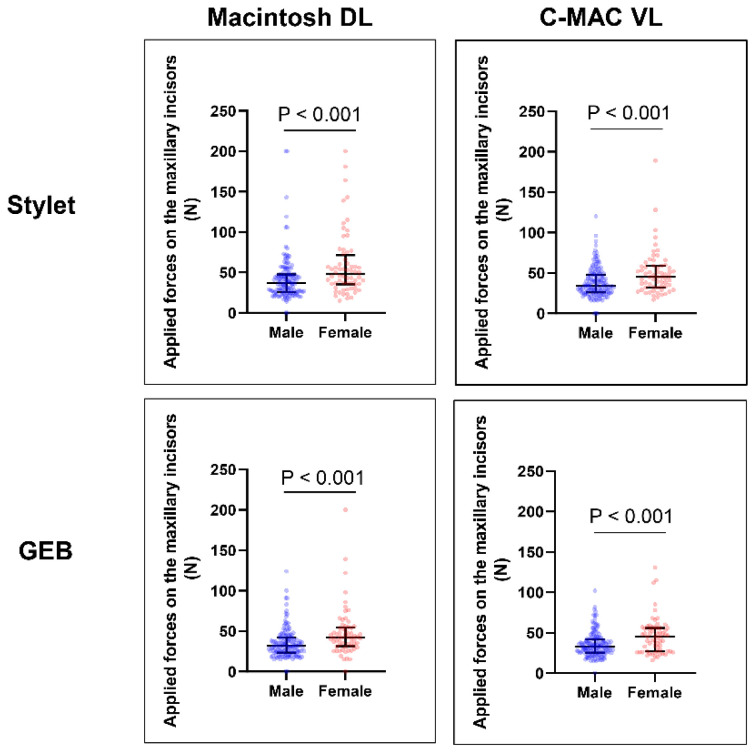
Endotracheal intubation (ETI) is a common and crucial intervention. Whether the performance of ETI differs according to the sex of the laryngoscopist remains unclear. The aim of this study was to assess sex disparities in markers of ETI performance among novices using a high-fidelity simulator. This prospective observational study was conducted from April 2017 to March 2019 in a public medical university. In total, 209 medical students (4th and 5th grade) without clinical ETI experience were recruited. Of the 209 students, 64 (30.6%) were female. The participants used either a Macintosh direct laryngoscope or C-MAC video laryngoscope in combination with a stylet or gum-elastic bougie to perform ETI on a high-fidelity simulator. The primary endpoint was the maximum force applied on the maxillary incisors during laryngoscopy. The secondary endpoint was the time to ETI. The implanted sensors in the simulator automatically quantified the force and time to ETI. The maximum force applied on the maxillary incisors was approximately 30% lower in the male than female group for all laryngoscopes and intubation aids examined (all P < 0.001). Similarly, the time to ETI was approximately 10% faster in the male than female group regardless of the types of laryngoscopes and intubation aids used (all P < 0.05). In this study, male sex was associated with a lower maximum force applied on the maxillary incisors during both direct and indirect laryngoscopy performed by novices. A clinical study focusing on sex differences in ETI performance is needed to validate our findings.
Keywords: Airway-related adverse events; Definitive airway management; Laryngoscopy; Medical student; Sex gap.
Figures




References
-
- Brown CA, 3rd, Bair AE, Pallin DJ, Walls RM NEAR III Investigators. Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med. 2015;65(4)(e1):363–370. - PubMed
-
- Hasegawa K, Shigemitsu K, Hagiwara Y, Chiba T, Watase H, Brown CA, 3rd, et al. Association between repeated intubation attempts and adverse events in emergency departments: an analysis of a multicenter prospective observational study. Ann Emerg Med. 2012;60(6)(e2):749–754. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous