

The Impact of State Medicaid Eligibility and Benefits Policy on Neonatal Abstinence Syndrome Hospitalizations
- PMID: 38463202
- PMCID: PMC10923531
- DOI: 10.1111/coep.12623
The Impact of State Medicaid Eligibility and Benefits Policy on Neonatal Abstinence Syndrome Hospitalizations
Abstract
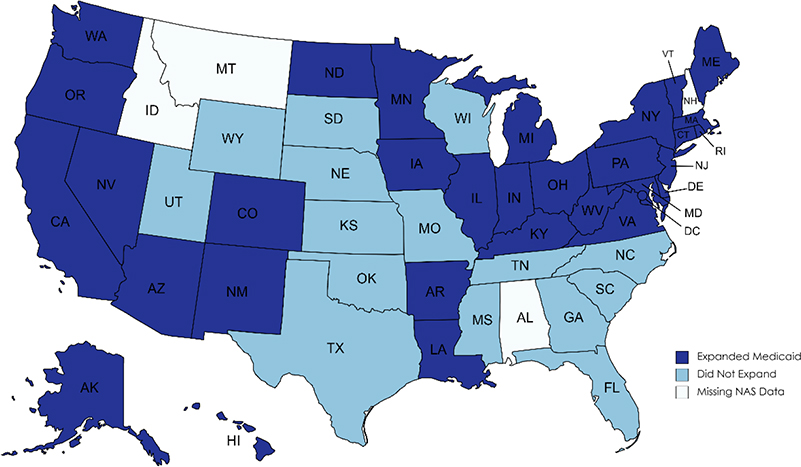
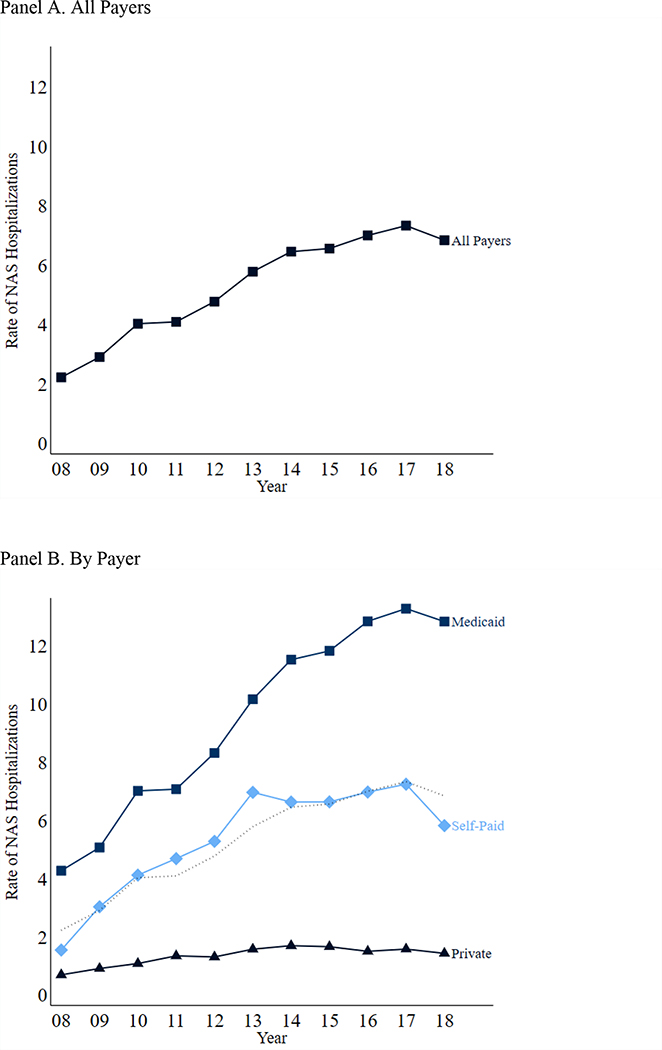
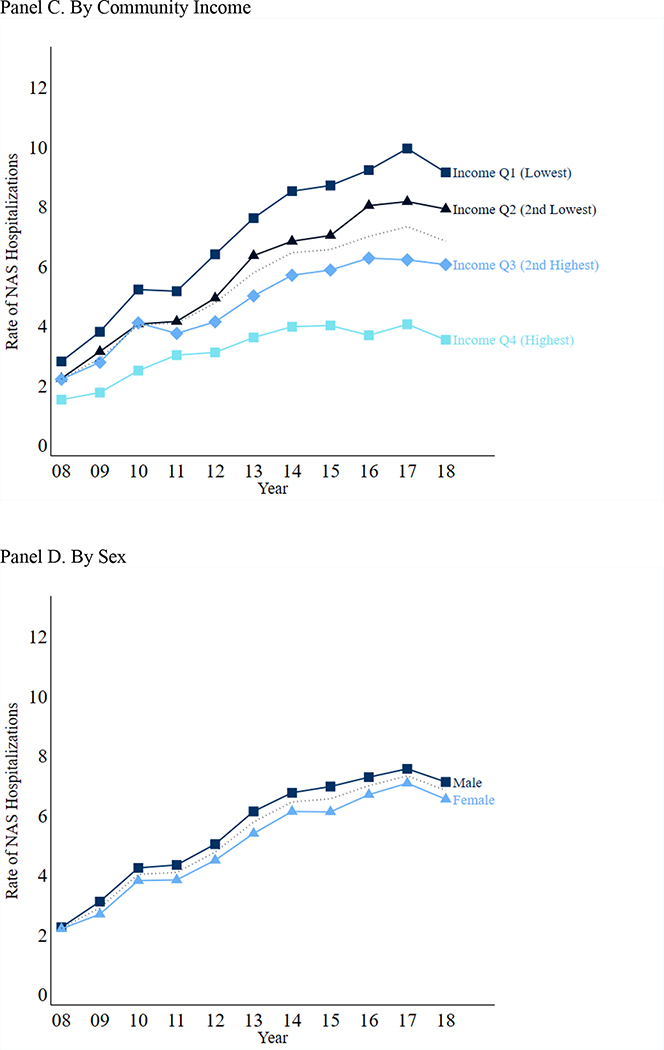
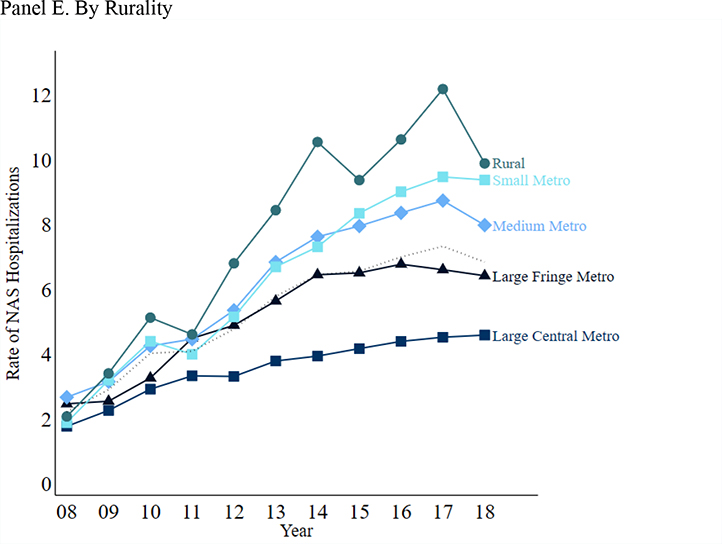
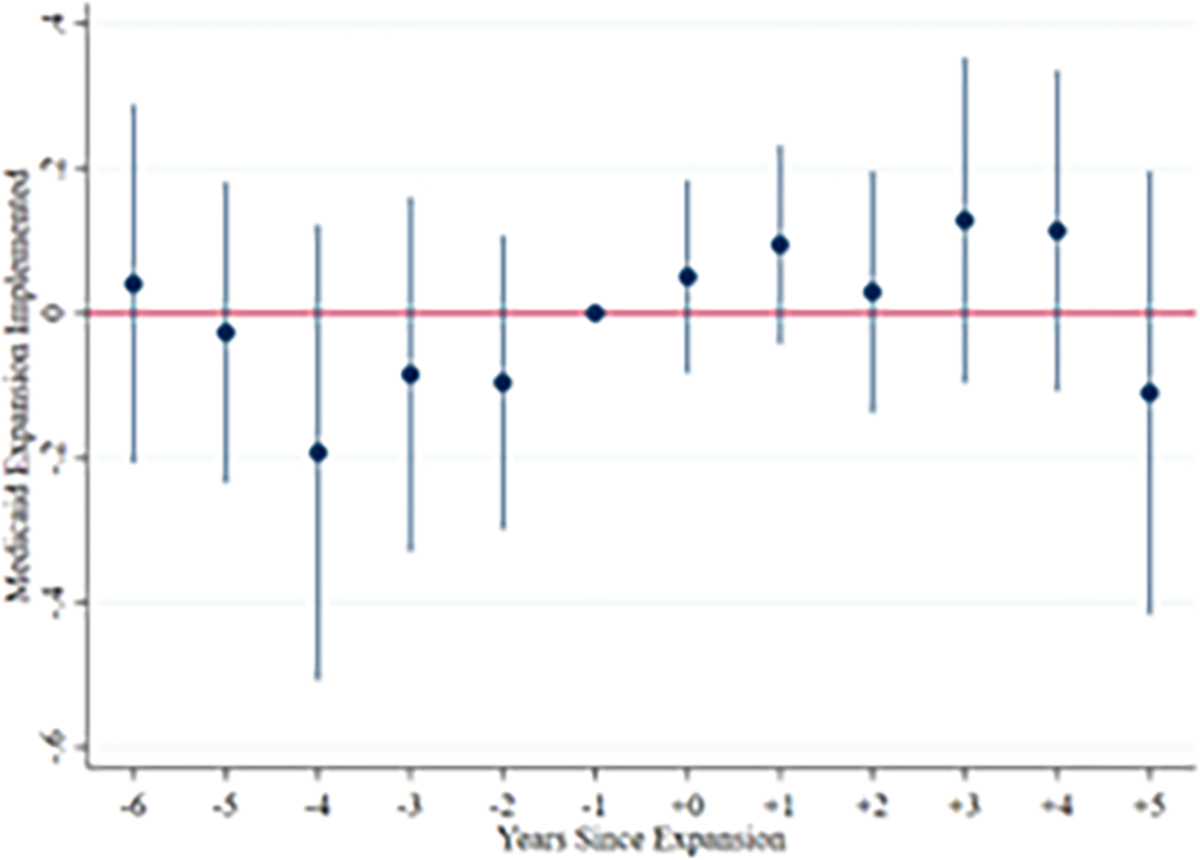
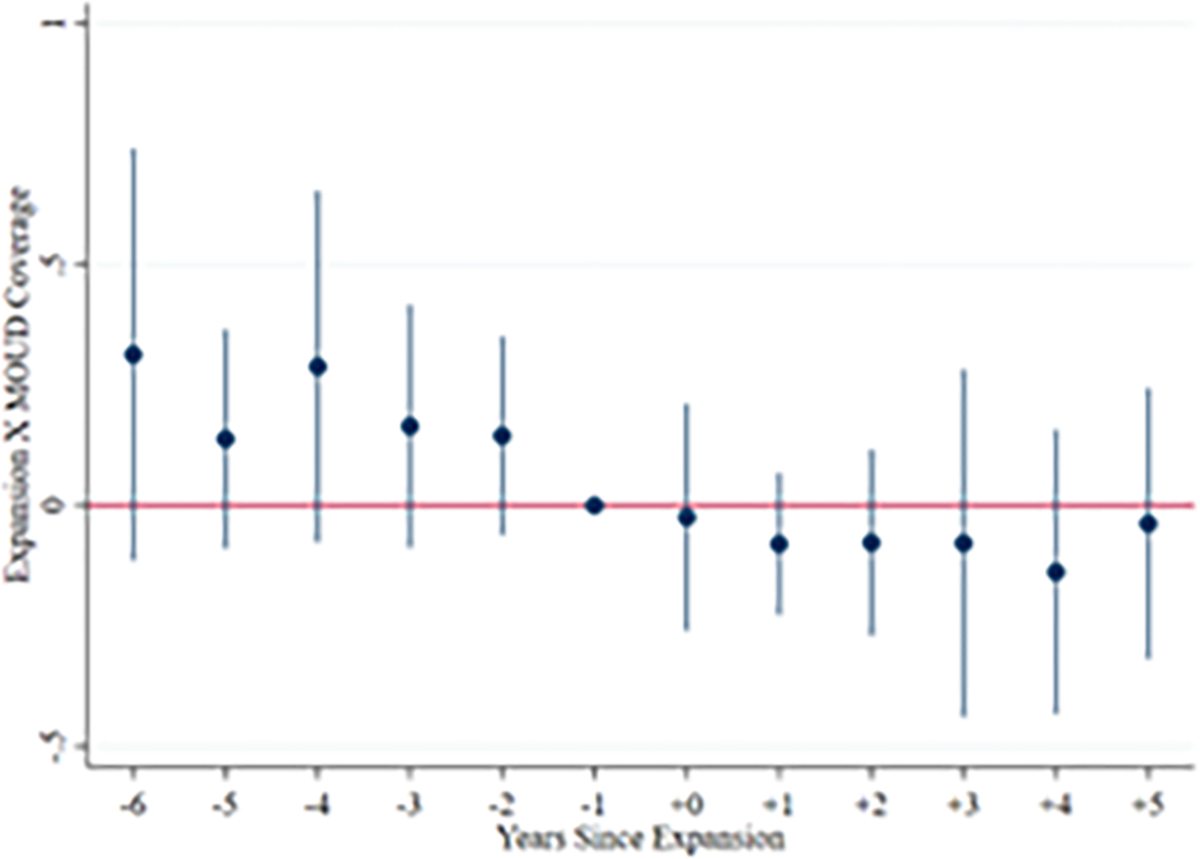
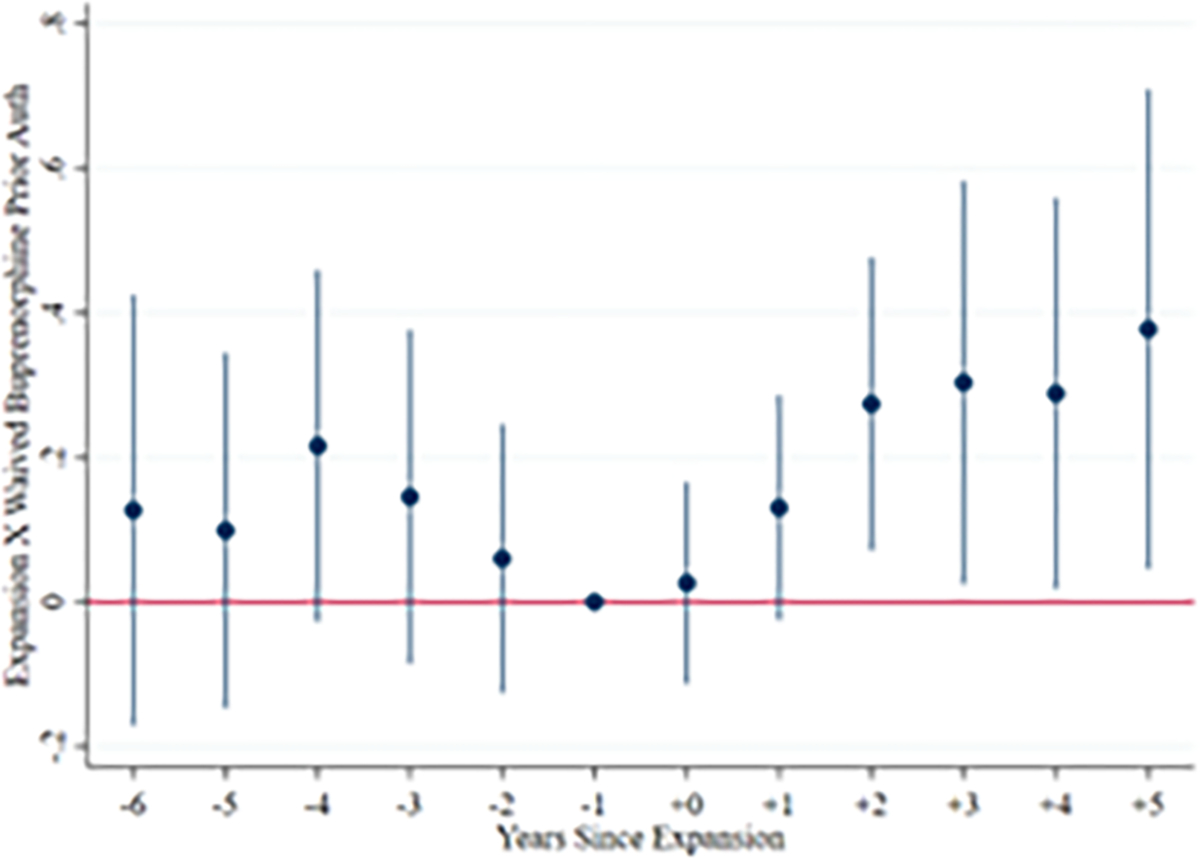
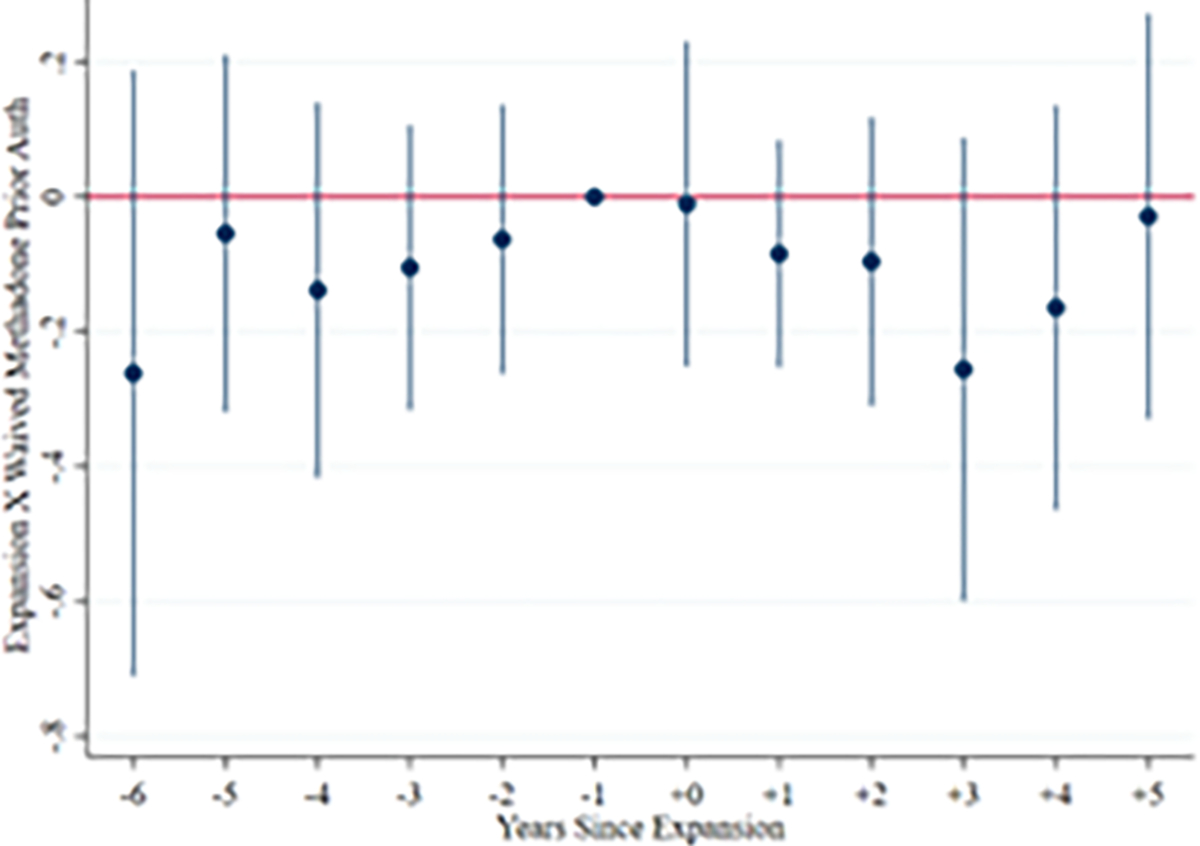
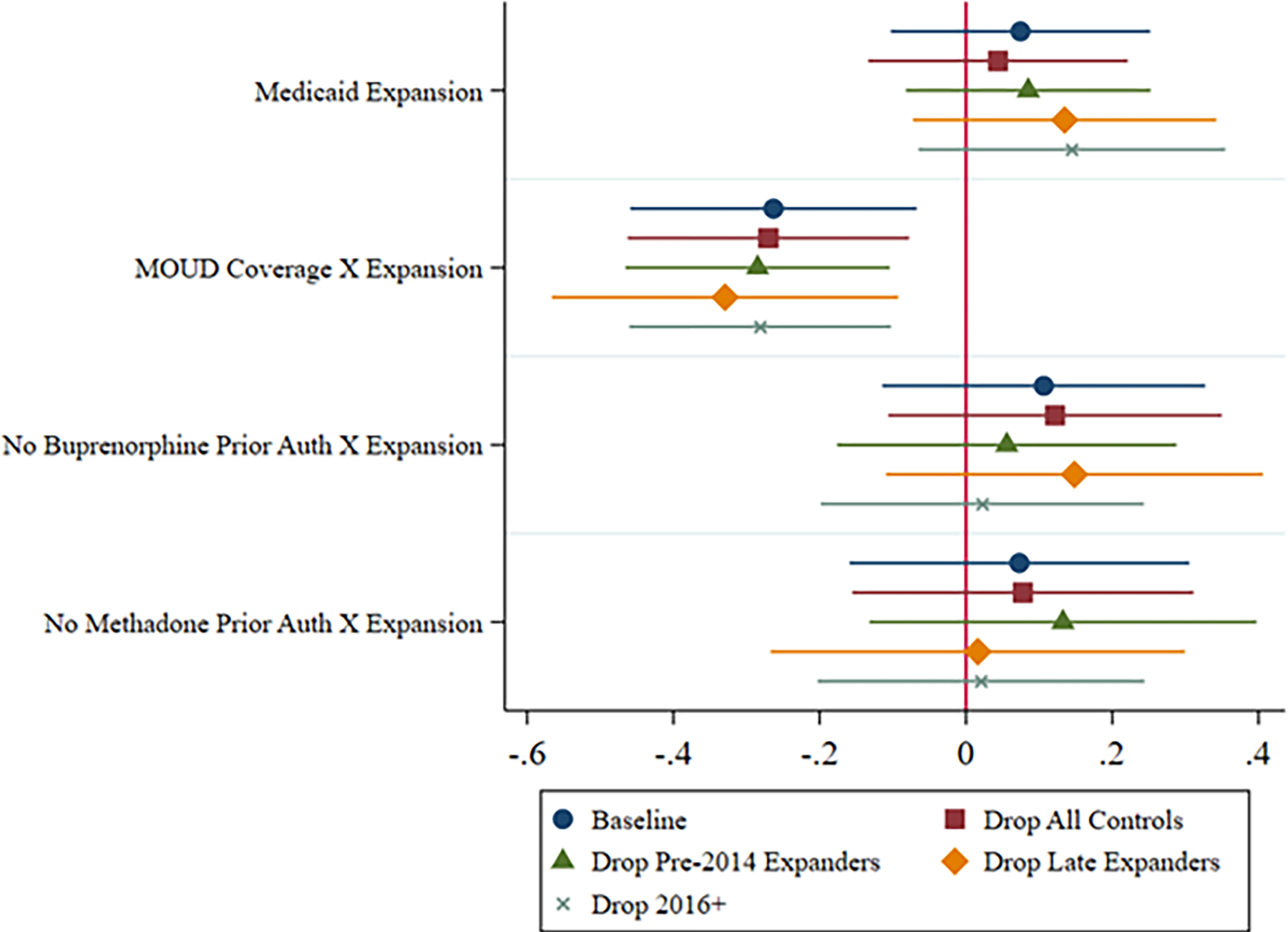
Rates of neonatal abstinence syndrome (NAS) resulting from opioid misuse are rising. However, policies to treat opioid misuse during pregnancy are unclear. We apply a difference-in-differences design to national pediatric discharge records to examine the effects of state Medicaid policies on NAS. Among states in which Medicaid covered two clinically-recommended medications for treating opioid misuse (buprenorphine, methadone), the Affordable Care Act's Medicaid expansion reduced Medicaid-covered NAS hospitalizations. Medicaid expansion did not affect NAS hospitalizations in other expansion states. These findings imply a nuanced relationship between Medicaid policy and NAS that should be considered in addressing opioid misuse among pregnant women.
Keywords: Medicaid; Neonatal abstinence syndrome; Opioids.
Conflict of interest statement
Conflict of Interest Statement: The authors have no known conflict of interest regarding the subject of this paper.
Figures
Similar articles
-
Association between punitive policies and neonatal abstinence syndrome among Medicaid-insured infants in complex policy environments.Addiction. 2022 Jan;117(1):162-171. doi: 10.1111/add.15602. Epub 2021 Jul 7. Addiction. 2022. PMID: 34096671 Free PMC article.
-
Prenatal Substance Exposure and Neonatal Abstinence Syndrome: State Estimates from the 2016-2020 Transformed Medicaid Statistical Information System.Matern Child Health J. 2023 Dec;27(Suppl 1):14-22. doi: 10.1007/s10995-023-03670-z. Epub 2023 May 23. Matern Child Health J. 2023. PMID: 37219692 Free PMC article.
-
Exposure to prescription opioid analgesics in utero and risk of neonatal abstinence syndrome: population based cohort study.BMJ. 2015 May 14;350:h2102. doi: 10.1136/bmj.h2102. BMJ. 2015. PMID: 25975601 Free PMC article.
-
Analgesia, Opioids, and Other Drug Use During Pregnancy and Neonatal Abstinence Syndrome.Clin Perinatol. 2019 Jun;46(2):349-366. doi: 10.1016/j.clp.2019.02.013. Epub 2019 Mar 30. Clin Perinatol. 2019. PMID: 31010564 Review.
-
Opioid treatment for opioid withdrawal in newborn infants.Cochrane Database Syst Rev. 2021 Jul 7;7(7):CD002059. doi: 10.1002/14651858.CD002059.pub4. Cochrane Database Syst Rev. 2021. PMID: 34231914 Free PMC article.
References
-
- American Society of Addiction Medicine. (2020). The ASAM National Practice Guideline for the Use of Medication in the Treatment of Addiction Involving Opioid Use: 2020 Focused Update. https://www.asam.org/docs/default-source/quality-science/npg-jam-supplem... - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources