

Correlation between serum markers and transjugular intrahepatic portosystemic shunt prognosis in patients with cirrhotic ascites
- PMID: 38463353
- PMCID: PMC10921209
- DOI: 10.4240/wjgs.v16.i2.481
Correlation between serum markers and transjugular intrahepatic portosystemic shunt prognosis in patients with cirrhotic ascites
Abstract
Background: Individuals with refractory ascites in the context of liver cirrhosis typically face an adverse prognosis. The transjugular intrahepatic portosystemic shunt (TIPS) is an efficacious intervention, but there is a lack of reliable tools for postoperative prognosis assessment. Previously utilized clinical biochemical markers, such as the serum albumin concentration (Alb), sodium (Na+) concentration, and serum creatinine (Scr), have limited predictive value. Therefore, the quest for novel, specific biomarkers to evaluate the post-TIPS prognosis in patients with liver cirrhosis and refractory ascites holds significant practical importance.
Aim: To investigate the associations between the Child-Pugh score, model for end-stage liver disease (MELD) score, and serum cystatin C (Cys C) level and post-TIPS prognosis in patients with liver cirrhosis and refractory ascites.
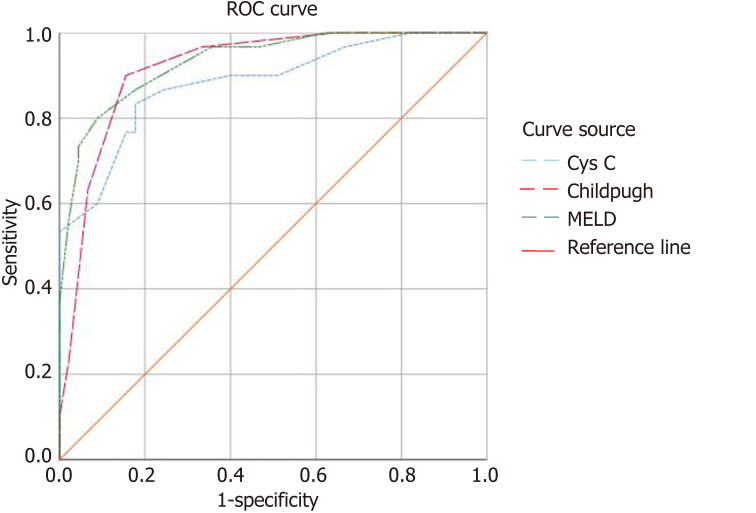
Methods: A retrospective analysis was conducted on 75 patients with liver cirrhosis and refractory ascites who underwent TIPS at our institution from August 2019 to August 2021. These patients were followed up regularly for two years, and the death toll was meticulously documented. The patients were allocated into a survival group (n = 45 patients) or a deceased group (n = 30 patients) based on their prognosis status. The clinical data of the two groups were collected, and Child-Pugh scores and MELD scores were calculated for analysis. Spearman correlation analysis was carried out to evaluate the correlation of prognosis with Child-Pugh grade, MELD score, and Cys C level. Additionally, a multiple-factor analysis utilizing the Cox proportional hazard model was used to identify independent risk factors affecting the post-TIPS prognosis of patients with liver cirrhosis and refractory ascites. The receiver operating characteristic curve (ROC) ascertained the predictive value of the Cys C concentration, Child-Pugh grade, and MELD score for the prognosis of liver cirrhosis with refractory ascites in post-TIPS patients.
Results: During a 2-year follow-up period, among 75 patients with liver cirrhosis and refractory ascites who underwent TIPS treatment, 30 patients (40.00%) passed away. The deceased cohort exhibited heightened aspartate aminotransferase, alanine aminotransferase, total bilirubin, Scr, prothrombin time, Cys C, international normalized ratio, Child-Pugh, and MELD scores compared to those of the survival cohort, while Alb and Na+ levels were attenuated in the deceased group (P < 0.05). Spearman analysis revealed moderate to high positive correlations between prognosis and Child-Pugh score, MELD score, and Cys C level (r = 0.709, 0.749, 0.671, P < 0.05). Multivariate analysis using the Cox proportional hazard model demonstrated that the independent risk factors for post-TIPS prognosis in patients with liver cirrhosis and refractory ascites were Cys C (HR = 3.802; 95%CI: 1.313-11.015), Child-Pugh (HR = 3.030; 95%CI: 1.858-4.943), and MELD (HR = 1.222; 95%CI: 1.073-1.393) scores. ROC analysis confirmed that, compared to those of the classic prognostic models for Child-Pugh and MELD scores, the predictive accuracy of Cys C for post-TIPS prognosis in patients with liver cirrhosis and refractory ascites was slightly lower. This analysis yielded sensitivity and specificity values of 83.33% and 82.22%, respectively. The area under the curve value at this juncture was 0.883, with an optimal cutoff value set at 1.95 mg/L.
Conclusion: Monitoring the serum Cys C concentration is valuable for assessing the post-TIPS prognosis in patients with liver cirrhosis and refractory ascites. Predictive models based on serum Cys C levels, as opposed to Scr levels, are more beneficial for evaluating the condition and prognosis of patients with ascites due to cirrhosis.
Keywords: Cystatin C; Liver cirrhosis; Refractory ascites; Transjugular intrahepatic portosystemic shunt.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
Similar articles
-
[MELD score in prediction of early mortality in patients suffering refractory ascites treated by TIPS].Vnitr Lek. 2006 Sep;52(9):771-6. Vnitr Lek. 2006. PMID: 17091599 Czech.
-
Child-Pugh versus MELD score in predicting survival in patients undergoing transjugular intrahepatic portosystemic shunt.Gut. 2003 Jun;52(6):879-85. doi: 10.1136/gut.52.6.879. Gut. 2003. PMID: 12740346 Free PMC article.
-
Combination of Model for End-Stage Liver Disease (MELD) and Sarcopenia predicts mortality after transjugular intrahepatic portosystemic shunt (TIPS).Dig Liver Dis. 2024 Sep;56(9):1544-1550. doi: 10.1016/j.dld.2024.03.003. Epub 2024 Mar 29. Dig Liver Dis. 2024. PMID: 38555198
-
Predictive Accuracy Comparison of Prognostic Scoring Systems for Survival in Patients Undergoing TIPS Placement: A Systematic Review and Meta-analysis.Acad Radiol. 2024 Sep;31(9):3688-3710. doi: 10.1016/j.acra.2023.10.050. Epub 2023 Nov 23. Acad Radiol. 2024. PMID: 38000922
-
The Role of Transjugular Intrahepatic Portosystemic Shunt for the Management of Ascites in Patients with Decompensated Cirrhosis.J Clin Med. 2024 Feb 27;13(5):1349. doi: 10.3390/jcm13051349. J Clin Med. 2024. PMID: 38592162 Free PMC article. Review.
References
-
- Wilson R, Williams DM. Cirrhosis. Med Clin North Am. 2022;106:437–446. - PubMed
-
- Bajaj JS, Kamath PS, Reddy KR. The Evolving Challenge of Infections in Cirrhosis. N Engl J Med. 2021;384:2317–2330. - PubMed
-
- Ginès P, Krag A, Abraldes JG, Solà E, Fabrellas N, Kamath PS. Liver cirrhosis. Lancet. 2021;398:1359–1376. - PubMed
-
- Karagiannakis DS, Voulgaris T, Siakavellas SI, Papatheodoridis GV, Vlachogiannakos J. Evaluation of portal hypertension in the cirrhotic patient: hepatic vein pressure gradient and beyond. Scand J Gastroenterol. 2018;53:1153–1164. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
