

Current clinical findings of acute neurological syndromes after SARS-CoV-2 infection
- PMID: 38463395
- PMCID: PMC10924641
- DOI: 10.1002/mco2.508
Current clinical findings of acute neurological syndromes after SARS-CoV-2 infection
Abstract
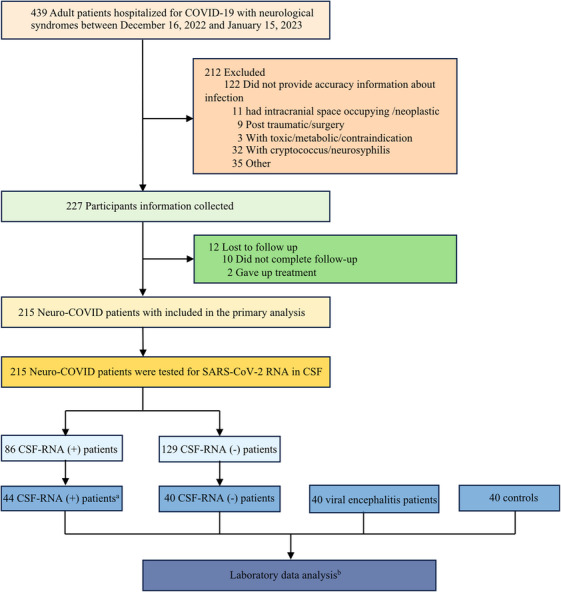
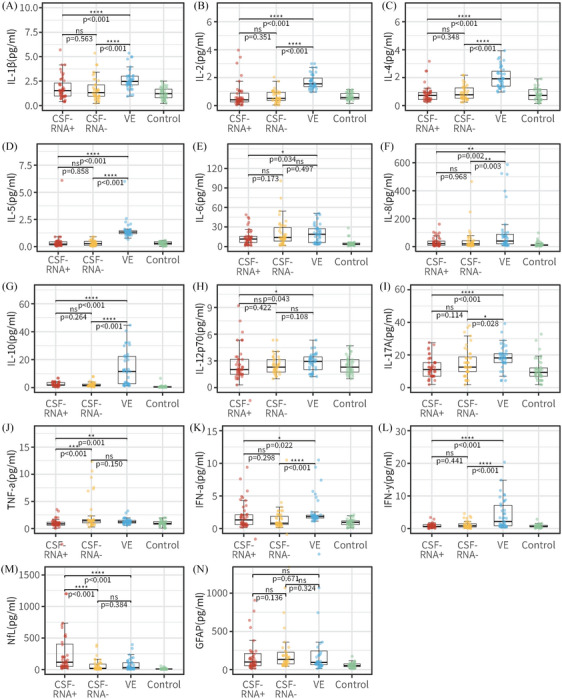
Neuro-COVID, a condition marked by persistent symptoms post-COVID-19 infection, notably affects various organs, with a particular focus on the central nervous system (CNS). Despite scant evidence of SARS-CoV-2 invasion in the CNS, the increasing incidence of Neuro-COVID cases indicates the onset of acute neurological symptoms early in infection. The Omicron variant, distinguished by heightened neurotropism, penetrates the CNS via the olfactory bulb. This direct invasion induces inflammation and neuronal damage, emphasizing the need for vigilance regarding potential neurological complications. Our multicenter study represents a groundbreaking revelation, documenting the definite presence of SARS-CoV-2 in the cerebrospinal fluid (CSF) of a significant proportion of Neuro-COVID patients. Furthermore, notable differences emerged between RNA-CSF-positive and negative patients, encompassing aspects such as blood-brain barrier integrity, extent of neuronal damage, and the activation status of inflammation. Despite inherent limitations, this research provides pivotal insights into the intricate interplay between SARS-CoV-2 and the CNS, underscoring the necessity for ongoing research to fully comprehend the virus's enduring effects on the CNS. The findings underscore the urgency of continuous investigation Neuro-COVID to unravel the complexities of this relationship, and pivotal in addressing the long-term consequences of COVID-19 on neurological health.
Keywords: Neuro‐COVID; SARS‐CoV‐2; central nerve injury; neurological syndromes; neurotropic invasion.
© 2024 The Authors. MedComm published by Sichuan International Medical Exchange & Promotion Association (SCIMEA) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous