

Development and Validation of a Novel Predictive Model for the Early Differentiation of Cardiac and Non-Cardiac Syncope
- PMID: 38463438
- PMCID: PMC10924787
- DOI: 10.2147/IJGM.S454521
Development and Validation of a Novel Predictive Model for the Early Differentiation of Cardiac and Non-Cardiac Syncope
Abstract
Background: The diagnosis of cardiac syncope remains a challenge. This study sought to develop and validate a diagnostic model for the early identification of individuals likely to have a cardiac cause.
Methods: 877 syncope patients with a determined cause were retrospectively enrolled at a tertiary heart center. They were randomly divided into the training set and validation set at a 7:3 ratio. We analyzed the demographic information, medical history, laboratory tests, electrocardiogram, and echocardiogram by the least absolute shrinkage and selection operator (LASSO) regression for selection of key features. Then a multivariable logistic regression analysis was performed to identify independent predictors and construct a diagnostic model. The receiver operating characteristic curves, area under the curve (AUC), calibration curves, and decision curve analysis were used to evaluate the predictive accuracy and clinical value of this nomogram.
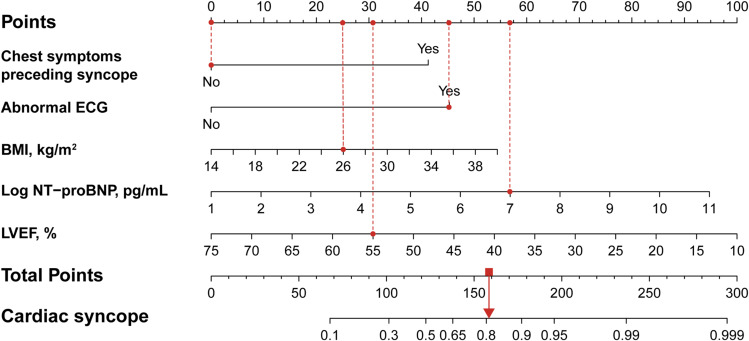
Results: Five independent predictors for cardiac syncope were selected: BMI (OR 1.088; 95% CI 1.022-1.158; P =0.008), chest symptoms preceding syncope (OR 5.251; 95% CI 3.326-8.288; P <0.001), logarithmic NT-proBNP (OR 1.463; 95% CI 1.240-1.727; P <0.001), left ventricular ejection fraction (OR 0.940; 95% CI 0.908-0.973; P <0.001), and abnormal electrocardiogram (OR 6.171; 95% CI 3.966-9.600; P <0.001). Subsequently, a nomogram based on a multivariate logistic regression model was developed and validated, yielding AUC of 0.873 (95% CI 0.845-0.902) and 0.856 (95% CI 0.809-0.903), respectively. The calibration curves showcased the nomogram's reasonable calibration, and the decision curve analysis demonstrated good clinical utility.
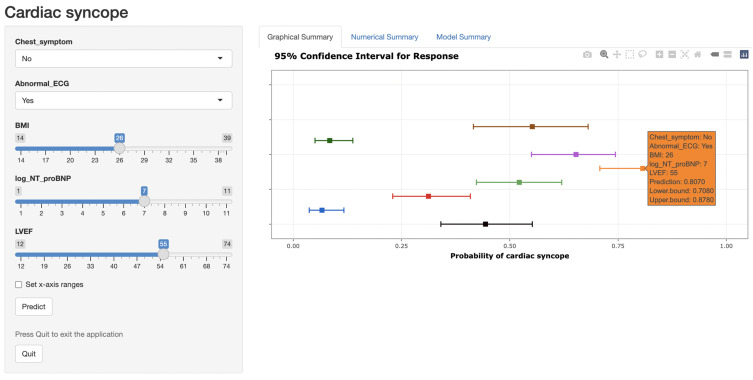
Conclusion: A diagnostic tool providing individualized probability predictions for cardiac syncope was developed and validated, which may potentially serve as an effective tool to facilitate early identification of such patients.
Keywords: cardiac syncope; diagnosis; nomogram; prediction model; syncope.
© 2024 Wu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures



Similar articles
-
Early identification of mild cognitive impairment: an innovative model using ocular biomarkers.Front Aging Neurosci. 2025 Apr 22;17:1492804. doi: 10.3389/fnagi.2025.1492804. eCollection 2025. Front Aging Neurosci. 2025. PMID: 40330593 Free PMC article.
-
A new prediction model for sustained ventricular tachycardia in arrhythmogenic cardiomyopathy.Front Cardiovasc Med. 2024 Dec 16;11:1477931. doi: 10.3389/fcvm.2024.1477931. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39736878 Free PMC article.
-
Establishment and Validation of a Non-invasive Diagnostic Nomogram to Identify Heart Failure in Patients With Coronary Heart Disease.Front Cardiovasc Med. 2022 Apr 7;9:875702. doi: 10.3389/fcvm.2022.875702. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35463796 Free PMC article.
-
Development and validation of a clinical prediction model for detecting coronary heart disease in middle-aged and elderly people: a diagnostic study.Eur J Med Res. 2023 Sep 25;28(1):375. doi: 10.1186/s40001-023-01233-0. Eur J Med Res. 2023. PMID: 37749613 Free PMC article.
-
Application of an individualized nomogram in first-trimester screening for trisomy 21.Ultrasound Obstet Gynecol. 2021 Jul;58(1):56-66. doi: 10.1002/uog.22087. Ultrasound Obstet Gynecol. 2021. PMID: 32438493 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
