

The role of multimodal ultrasound in diagnosis of fetal bowel dilatation and prediction of adverse neonatal outcomes: A study of 86 cases in a series of 43,562 births
- PMID: 38463772
- PMCID: PMC10923836
- DOI: 10.1016/j.heliyon.2024.e27455
The role of multimodal ultrasound in diagnosis of fetal bowel dilatation and prediction of adverse neonatal outcomes: A study of 86 cases in a series of 43,562 births
Abstract
Objective: To investigate the diagnostic utility of multimodal ultrasound for fetal bowel dilatation (FBD) in different parts of the bowel and to examine its prognostic potential in FBD.
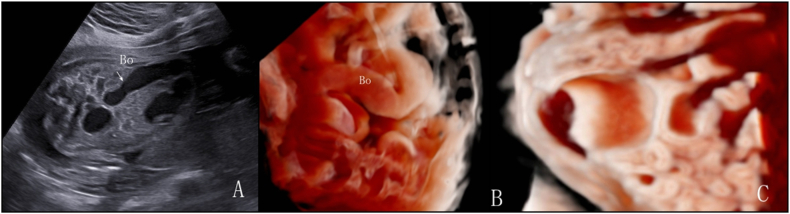
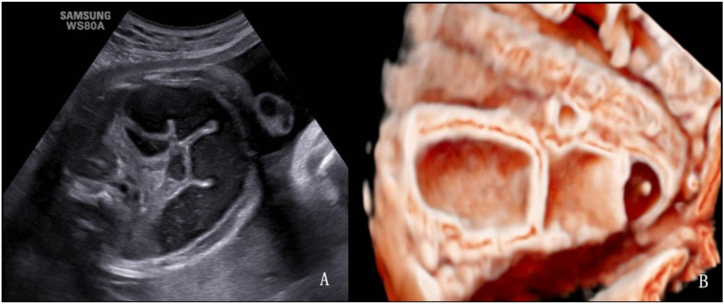
Methods: This retrospective study analyzed 86 fetuses with a dilated bowel identified via ultrasound in a 10-month postnatal follow-up. Both two- and three dimensional (2D and 3D, respectively) ultrasound volume imaging were used to characterize dilation across different bowel sections. The optimal intestinal diameter cut-off values for pathological bowel dilatation were determined and a predictive model for neonatal surgery was developed.
Results: The 86 cases of dilatation were distributed as follows: duodenal (n = 36); jejunum/ileum (n = 35); and colonic (n = 15). Duodenal dilatations presented the earliest during pregnancy compared to the other 2 groups (24.4 versus [vs.] 29 vs. 33.7 weeks respectively; p < 0.05). Cases with small intestinal dilatation were delivered earlier than those with colonic dilatation (p < 0.05). Infants with duodenal dilatation had the lowest birth weight and the highest rate of multi-system abnormalities (30.6% vs. 5.7% vs. 20%; p < 0.001). More than one-half of the multi-system abnormalities had chromosomal abnormalities (multiple, 54% vs. single, 12.5%; p = 0.015). There were 2 stillbirths, 24 induced labors, 44 postnatal surgeries, and 18 normal cases after birth. In predicting adverse neonatal outcomes of jejunum/ileum dilatation using a cut-off value of 15.5 mm small intestine diameter, sensitivity was 81.5%, specificity was 62.5%, and the area under the receiver operating characteristic curve (AUC) was 0.762 (p < 0.05). For colonic dilatation, using a cut-off value of 21.5 mm colon diameter: sensitivity was 83.3%, specificity was 77.8%, and AUC was 0.861 (p < 0.05). In detecting jejunum/ileum and colonic obstruction, 3D ultrasound demonstrated significantly better diagnostic efficiency than 2D ultrasound (p < 0.05). Using the backward stepwise selection method, a predictive model for neonatal surgery in patients with jejunum/ileum and colonic dilatation was established: logit (P) = -1.58 + (2.32 × polyhydramnios) +(2.0 × ascites) +(1.14 × hyperechogenic bowel). The AUC for the prediction model was 0.874 (p < 0.05), with 76% sensitivity and 94.1% specificity.
Conclusions: Duodenal dilatation occurred earlier, with a higher incidence of chromosomal abnormalities and multi-system abnormalities than dilatation of other parts of the bowel. 3D ultrasound played an important role in the detection of jejunum/ileum and colon obstructions. Clinical signs, including polyhydramnios, ascites, and strong echoes in the intestine, can be used to predict neonatal surgery.
Keywords: 3D ultrasound volume imaging; Fetal bowel dilatation; Multimodal ultrasound; Prediction model; Prenatal diagnosis.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures










Similar articles
-
Analysis of the clinical outcomes of fetal bowel dilatation combined with other abnormal ultrasonographic features.J Matern Fetal Neonatal Med. 2019 Mar;32(6):992-996. doi: 10.1080/14767058.2017.1397123. Epub 2017 Nov 7. J Matern Fetal Neonatal Med. 2019. PMID: 29113511
-
Fetal gastroschisis: a comparison of second vs. third-trimester bowel dilatation for predicting bowel atresia and neonatal outcomes.Ultraschall Med. 2013 Apr;34(2):157-61. doi: 10.1055/s-0031-1281753. Epub 2011 Dec 9. Ultraschall Med. 2013. PMID: 22161619
-
Diagnostic Accuracy of Prenatal Ultrasound in Identifying Jejunal and Ileal Atresia.Fetal Diagn Ther. 2015;38(2):142-6. doi: 10.1159/000368603. Epub 2015 Jan 21. Fetal Diagn Ther. 2015. PMID: 25613369
-
Role of magnetic resonance imaging in fetuses with mild or moderate ventriculomegaly in the era of fetal neurosonography: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2019 Aug;54(2):164-171. doi: 10.1002/uog.20197. Epub 2019 Jul 11. Ultrasound Obstet Gynecol. 2019. PMID: 30549340
-
Second-trimester intra-abdominal bowel dilation in fetuses with gastroschisis predicts neonatal bowel atresia.Ultrasound Obstet Gynecol. 2006 Nov;28(6):821-5. doi: 10.1002/uog.2858. Ultrasound Obstet Gynecol. 2006. PMID: 17029299 Review.
References
LinkOut - more resources
Full Text Sources
