

Mitochondrial DNA levels in perfusate and bile during ex vivo normothermic machine correspond with donor liver quality
- PMID: 38463874
- PMCID: PMC10920371
- DOI: 10.1016/j.heliyon.2024.e27122
Mitochondrial DNA levels in perfusate and bile during ex vivo normothermic machine correspond with donor liver quality
Abstract
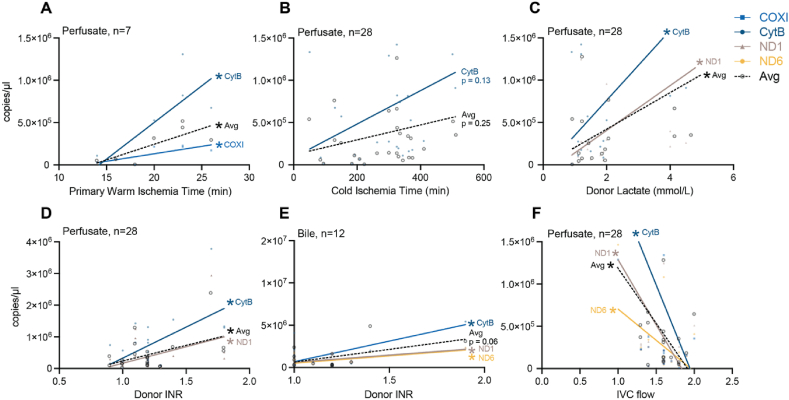
Ex vivo normothermic machine perfusion (NMP) preserves donor organs and permits real-time assessment of allograft health, but the most effective indicators of graft viability are uncertain. Mitochondrial DNA (mtDNA), released consequent to traumatic cell injury and death, including the ischemia-reperfusion injury inherent in transplantation, may meet the need for a biomarker in this context. We describe a real time PCR-based approach to assess cell-free mtDNA during NMP as a universal biomarker of allograft quality. Measured in the perfusate fluid of 29 livers, the quantity of mtDNA correlated with metrics of donor liver health including International Normalized Ratio (INR), lactate, and warm ischemia time, and inversely correlated with inferior vena cava (IVC) flow during perfusion. Our findings endorse mtDNA as a simple and rapidly measured feature that can inform donor liver health, opening the possibility to better assess livers acquired from extended criteria donors to improve organ supply.
Keywords: Extended criteria organ donation; Liver transplantation; Mitochondrial DAMPs; Mitochondrial DNA; Normothermic organ perfusion; Organ health assessment; Solid organ transplantation.
© 2024 The Authors.
Conflict of interest statement
The authors declare that no conflict of interest exists.
Figures



References
-
- Pandya K., Sastry V., Panlilio M.T., Yip T.C.F., Salimi S., West C., Virtue S., Wells M., Crawford M., Pulitano C., et al. Differential impact of extended criteria donors after brain death or circulatory death in adult liver transplantation. Liver Transplant. 2020;26:1603–1617. doi: 10.1002/lt.25859. - DOI - PubMed
LinkOut - more resources
Full Text Sources
