

This is a preprint.
Association of Long-Term Blood Pressure Variability with Cerebral Amyloid Angiopathy-related Brain Injury and Cognitive Decline
- PMID: 38464316
- PMCID: PMC10925352
- DOI: 10.1101/2024.02.24.24303071
Association of Long-Term Blood Pressure Variability with Cerebral Amyloid Angiopathy-related Brain Injury and Cognitive Decline
Abstract
Introduction: Long-term systolic blood pressure variability (BPV) has been proposed as a novel risk factor for dementia, but the underlying mechanisms are largely unknown. We aimed to investigate the association between long-term blood pressure variability (BPV), brain injury, and cognitive decline in patients with mild cognitive symptoms and cerebral amyloid angiopathy (CAA), a well-characterized small-vessel disease that causes cognitive decline in older adults.
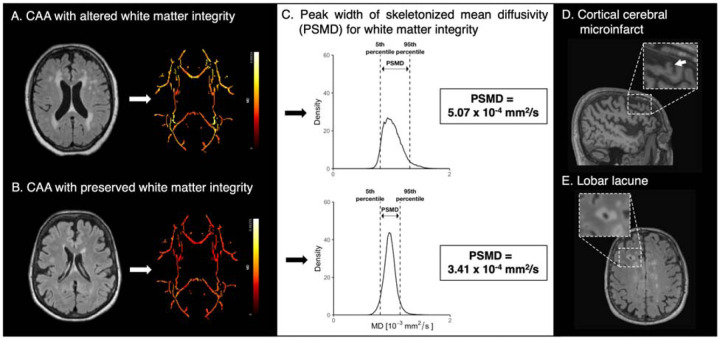
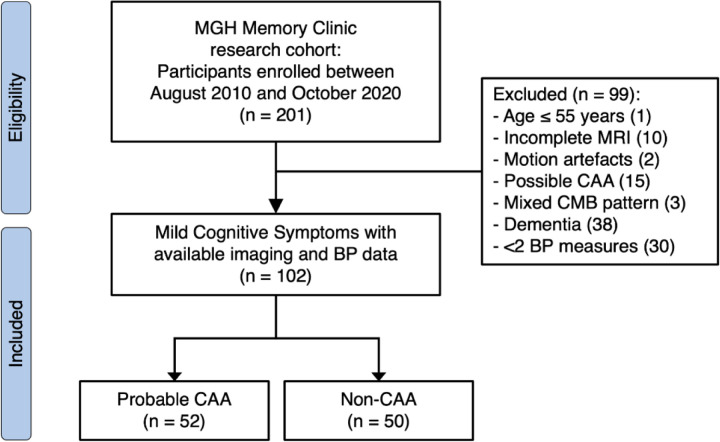
Methods: Using a prospective memory clinic cohort, we enrolled 102 participants, of whom 52 with probable CAA. All underwent a 3-tesla research MRI at baseline and annual neuropsychological evaluation over 2 years, for which standardized z-scores for four cognitive domains were calculated. BPV was assessed using a coefficient of variation derived from serial outpatient BP measurements (median 12) over five years. We measured the peak width of skeletonized mean diffusivity (PSMD) as a marker of white matter integrity, and other neuroimaging markers of CAA, including lacunes and cortical cerebral microinfarcts. Using regression models, we evaluated the association of BPV with microstructural brain injury and whether CAA modified this association. We also examined the association of BPV with subsequent cognitive decline.
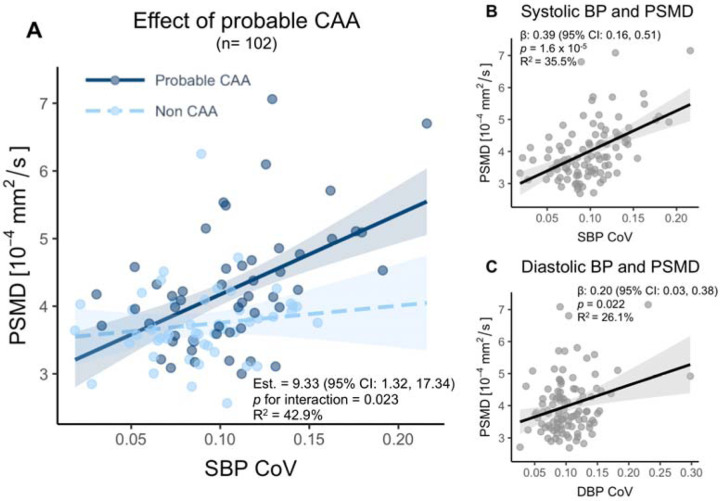
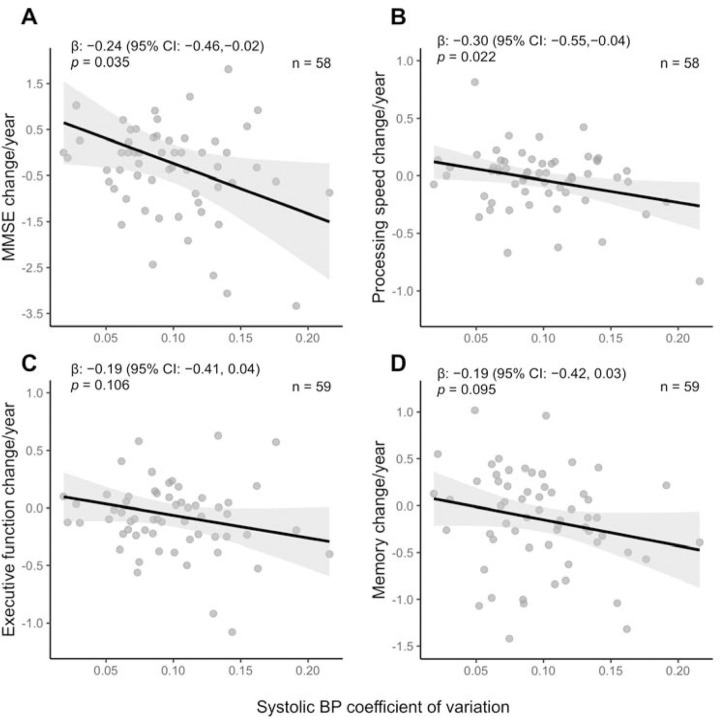
Results: Systolic BPV was dose-dependently associated with PSMD (estimate=0.22, 95% CI: 0.06, 0.39, p=0.010), independent of age, sex, mean BP, common vascular risk factors, brain atrophy, and CAA severity. The presence of probable CAA strengthened the association between BPV and PSMD (estimate=9.33, 95% CI: 1.32, 17.34, p for interaction = 0.023). Higher BPV correlated with greater ischemic injury (lobar lacunes and cortical cerebral microinfarcts) and a decline in global cognition and processing speed (estimate=-0.30, 95% CI: -0.55, -0.04, p=0.022).
Discussion: Long-term BPV has a dose-dependent association with alterations in white matter integrity, lobar lacunes, and cortical cerebral microinfarcts, and predicts cognitive decline. Controlling BPV is a potential strategic approach to prevent cognitive decline, especially in early-stage CAA.
Keywords: Alzheimer’s Disease; Blood pressure variability; Cerebral amyloid angiopathy; Cerebrovascular disease/Stroke; MCI (mild cognitive impairment); Vascular Dementia.
Conflict of interest statement
Conflicts of interest The authors report no conflicts of interest relevant to the manuscript.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources