

The Burden and Impact of Early Post-transplant Multidrug-Resistant Organism Detection Among Renal Transplant Recipients, 2005-2021
- PMID: 38464488
- PMCID: PMC10924447
- DOI: 10.1093/ofid/ofae060
The Burden and Impact of Early Post-transplant Multidrug-Resistant Organism Detection Among Renal Transplant Recipients, 2005-2021
Erratum in
-
Correction to: The Burden and Impact of Early Post-transplant Multidrug-Resistant Organism Detection Among Renal Transplant Recipients, 2005-2021.Open Forum Infect Dis. 2024 Sep 20;11(9):ofae541. doi: 10.1093/ofid/ofae541. eCollection 2024 Sep. Open Forum Infect Dis. 2024. PMID: 39310273 Free PMC article.
Abstract
Background: Reducing the burden of multidrug-resistant organism (MDRO) colonization and infection among renal transplant recipients (RTRs) may improve patient outcomes. We aimed to assess whether the detection of an MDRO or a comparable antibiotic-susceptible organism (CSO) during the early post-transplant (EPT) period was associated with graft loss and mortality among RTRs.
Methods: We conducted a retrospective cohort study of RTRs transplanted between 2005 and 2021. EPT positivity was defined as a positive bacterial culture within 30 days of transplant. The incidence and prevalence of EPT MDRO detection were calculated. The primary outcome was a composite of 1-year allograft loss or mortality following transplant. Multivariable Cox hazard regression, competing risk, propensity score-weighted sensitivity, and subgroup analyses were performed.
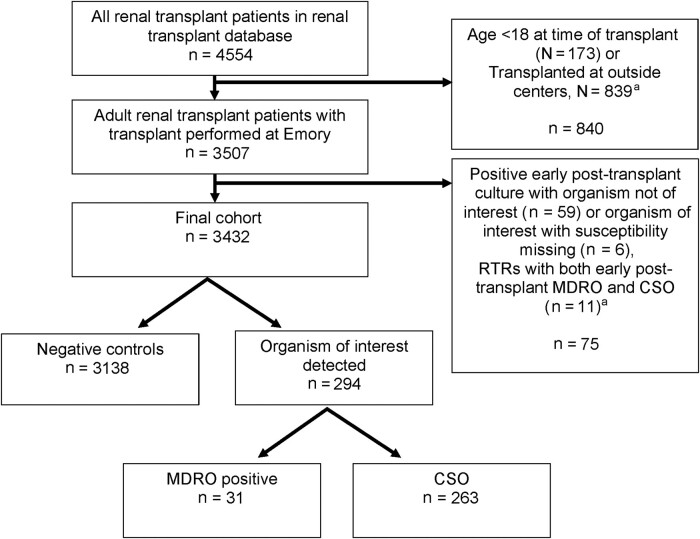
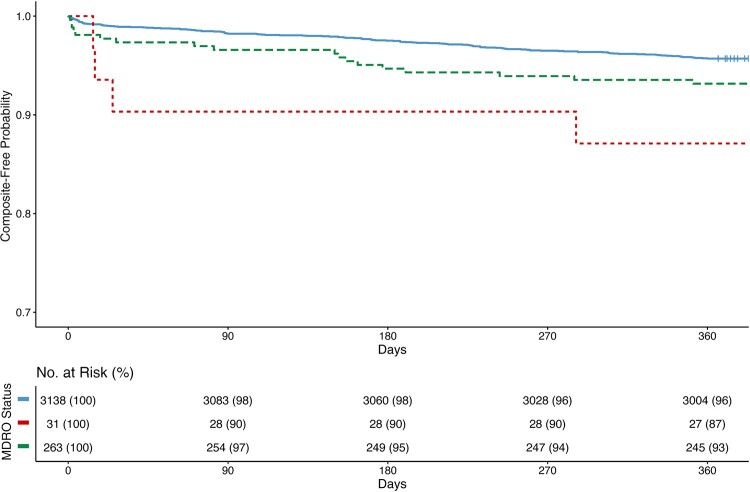
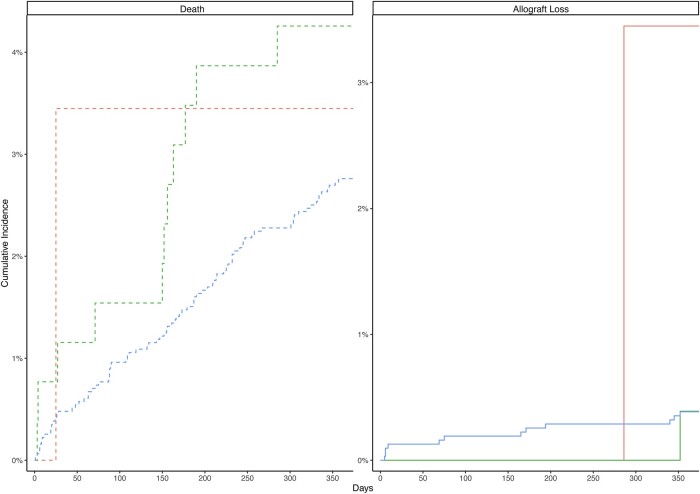
Results: Among 3507 RTRs, the prevalence of EPT MDRO detection was 1.3% (95% CI, 0.91%-1.69%) with an incidence rate per 1000 EPT-days at risk of 0.42 (95% CI, 0.31-0.57). Among RTRs who met survival analysis inclusion criteria (n = 3432), 91% (3138/3432) had no positive EPT cultures and were designated as negative controls, 8% (263/3432) had a CSO detected, and 1% (31/3432) had an MDRO detected in the EPT period. EPT MDRO detection was associated with the composite outcome (adjusted hazard ratio [aHR], 3.29; 95% CI, 1.21-8.92) and death-censored allograft loss (cause-specific aHR, 7.15; 95% CI, 0.92-55.5; subdistribution aHR, 7.15; 95% CI, 0.95-53.7). A similar trend was seen in the subgroup and sensitivity analyses.
Conclusions: MDRO detection during the EPT period was associated with allograft loss, suggesting the need for increased strategies to optimize prevention of MDRO colonization and infection.
Keywords: MDROs; allograft failure; renal transplant.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. A.B. has served on a clinical advisory board for Beckman Coulter. All other authors: no reported conflicts.
Figures
References
-
- Centers for Disease Control and Prevention . Antibiotic Resistance Threats in the United States. US Department of Health and Human Services, Centers for Disease Control and Prevention; 2019.
-
- World Health Organization . Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discover, and Development of New Antibiotics. World Health Organization; 2017.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
