

Association of Pre-PCI Blood Pressure and No-Reflow in Patients with Acute ST-Elevation Coronary Infarction
- PMID: 38464557
- PMCID: PMC10921965
- DOI: 10.5334/gh.1309
Association of Pre-PCI Blood Pressure and No-Reflow in Patients with Acute ST-Elevation Coronary Infarction
Abstract
Background: Previous studies have established blood pressure (BP) as a pivotal factor influencing no-reflow following primary percutaneous coronary intervention (PCI) in patients with ST-elevation acute coronary infarction (STEMI). However, no relevant study has been conducted to investigate the optimal range of BP associated with the lowest risk of no-reflow among STEMI patients so far. Therefore, our objective was to evaluate the association between pre-PCI BP and the occurrence of no-reflow in patients with STEMI.
Method: We included 1025 STEMI patients undergoing primary PCI. The BP pre-PCI was categorized into 20-mmHg increments. Logistic models were employed to assess the association of no-reflow with systolic blood pressure (SBP) or diastolic blood pressure (DBP). Three sensitivity analyses were conducted to further confirm the robustness of the association between blood pressure and no-reflow.
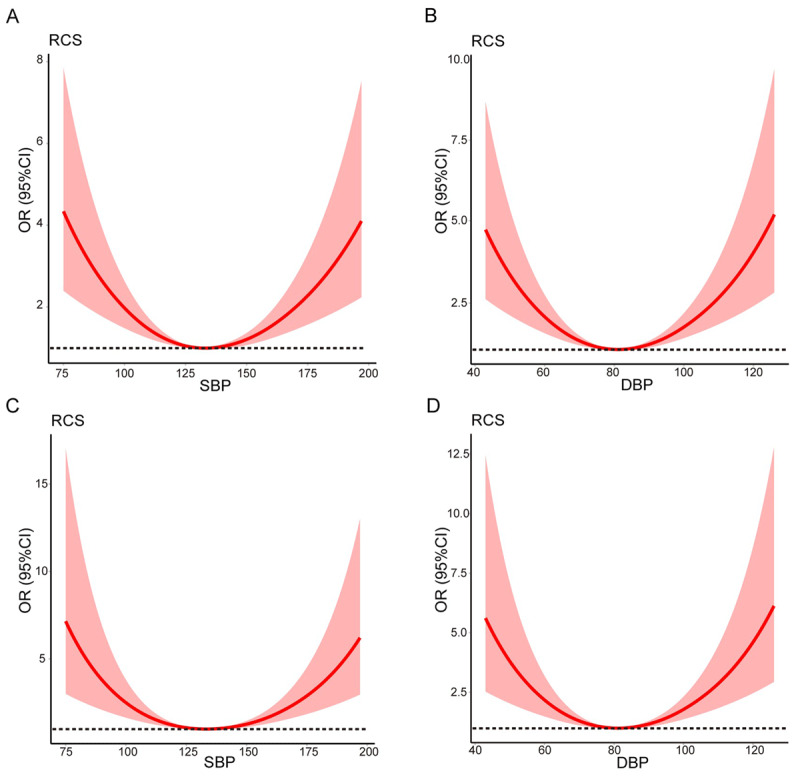
Results: SBP or DBP exhibited a U-shaped curve association with no-reflow. No-reflow was higher in patients with lower SBP (<100 mmHg) (adjusted hazard ratio (OR) 3.64, 95% confidence interval (CI) 1.84,7.21; p < 0.001) and lower DBP (<60 mmHg) (OR 3.28, 95% CI 1.63,6.49; p < 0.001) [reference: 120 ≤SBP <140; 80 ≤DBP <100 mmHg], respectively. Furthermore, no-reflow was higher in patients with higher SBP (≥160 mmHg) (OR 2.07, 95% CI 1.27,3.36; p = 0.003) and DBP (≥100 mmHg) (OR 3.36, 95% CI 2.07,5.46; p < 0.001), respectively. The results of sensitivity analyses were consistent with the above findings.
Conclusion: Maintaining a pre-PCI SBP within the range of 120 to 140 mmHg and a DBP within the range of 80 to 100 mmHg may be confer benefits to patients with STEMI in no-reflow.
Keywords: DBP (Diastolic blood pressure); SBP (Systolic blood pressure); STEMI (ST-elevation acute coronary infarction); no-reflow.
Copyright: © 2024 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
Similar articles
-
Predictors of no-reflow phenomenon following percutaneous coronary intervention for ST-segment elevation myocardial infarction.Ann Cardiol Angeiol (Paris). 2021 Jun;70(3):136-142. doi: 10.1016/j.ancard.2021.04.004. Epub 2021 May 4. Ann Cardiol Angeiol (Paris). 2021. PMID: 33962782
-
[Comparison of the predictive value of the modified CADILLAC, GRACE and TIMI risk scores for the risk of short-term death in patients with acute ST segment elevation myocardial infarction after percutaneous coronary intervention].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Mar;35(3):299-304. doi: 10.3760/cma.j.cn121430-20220727-00696. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 36916344 Chinese.
-
Coronary artery ectasia, an independent predictor of no-reflow after primary PCI for ST-elevation myocardial infarction.Int J Cardiol. 2018 Aug 15;265:12-17. doi: 10.1016/j.ijcard.2018.04.120. Epub 2018 Apr 25. Int J Cardiol. 2018. PMID: 29731349
-
The predictive value of laboratory parameters for no-reflow phenomenon in patients with ST-elevation myocardial infarction following primary percutaneous coronary intervention: A meta-analysis.Clin Cardiol. 2024 Feb;47(2):e24238. doi: 10.1002/clc.24238. Clin Cardiol. 2024. PMID: 38400562 Free PMC article. Review.
-
No reflow phenomenon in percutaneous coronary interventions in ST-segment elevation myocardial infarction.Indian Heart J. 2016 Jul-Aug;68(4):539-51. doi: 10.1016/j.ihj.2016.04.006. Epub 2016 Apr 19. Indian Heart J. 2016. PMID: 27543480 Free PMC article. Review.
Cited by
-
The HALP score predicts no-reflow phenomenon and long-term prognosis in patients with ST-segment elevation myocardial infarction after primary percutaneous coronary intervention.Coron Artery Dis. 2025 Jun 1;36(4):273-280. doi: 10.1097/MCA.0000000000001446. Epub 2024 Nov 4. Coron Artery Dis. 2025. PMID: 39492724 Free PMC article.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018; 39: 119–177. DOI: 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Fan F, Li Y, Zhang Y, Liu J, Hao Y, Smith SC Jr., Fonarow GC, Taubert KA, Ge J, Zhao D, Huo Y. CCC-ACS Investigators; Chest pain center accreditation is associated with improved in-hospital outcomes of acute myocardial infarction patients in China: Findings from the CCC-ACS Project. J Am Heart Assoc. 2019; 8: e002317. DOI: 10.1161/jaha.118.002317 - DOI - PMC - PubMed
-
- Chandrashekhar Y, Alexander T, Mullasari A, Kumbhani DJ, Alam S, Alexanderson E, Bachani D, Wilhelmus Badenhorst JC, Baliga R, Bax JJ, et al. Resource and infrastructure-appropriate management of ST-segment elevation myocardial infarction in low- and middle-income countries. Circulation. 2020; 141: 2004–2025. DOI: 10.1161/circulationaha.119.041297 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
