

The neurological wake-up test in severe pediatric traumatic brain injury: a long term, single-center experience
- PMID: 38464893
- PMCID: PMC10920253
- DOI: 10.3389/fped.2024.1367337
The neurological wake-up test in severe pediatric traumatic brain injury: a long term, single-center experience
Abstract
Objectives: To describe the use and outcomes of the neurological wake-up test (NWT) in pediatric severe traumatic brain injury (pTBI).
Design: Retrospective single-center observational cohort study.
Setting: Medical-surgical tertiary pediatric intensive care unit (PICU) in a university medical center and Level 1 Trauma Center.
Patients: Children younger than 18 years with severe TBI [i.e., Glasgow Coma Scale (GCS) of ≤8] admitted between January 2010 and December 2020. Subjects with non-traumatic brain injury were excluded.
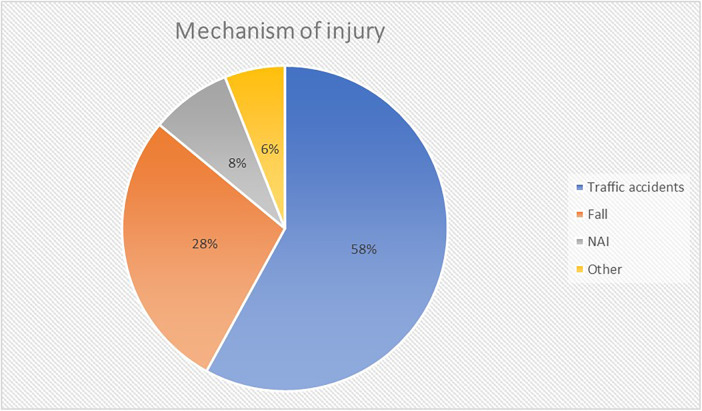
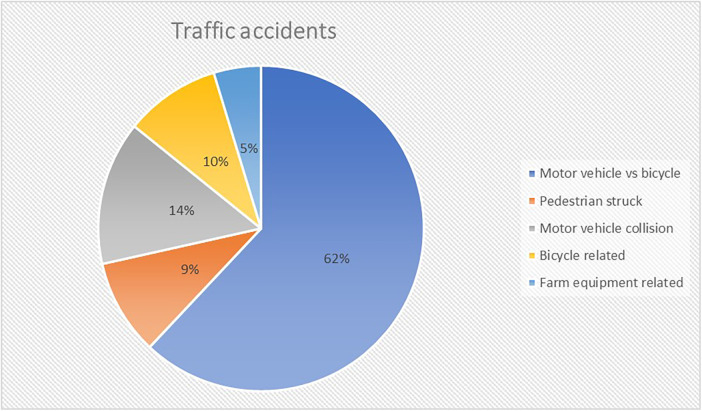
Measurements and main results: Of 168 TBI patients admitted, 36 (21%) met the inclusion criteria. Median age was 8.5 years [2 months to 16 years], 5 patients were younger than 6 months. Median initial Glasgow Coma Scale (GCS) and Glasgow Motor Scale (GMS) was 6 [3-8] and 3 [1-5]. NWTs were initiated in 14 (39%) patients, with 7 (50%) labelled as successful. Fall from a height was the underlying injury mechanism in those seven. NWT-failure occurred in patients admitted after traffic accidents. Sedation use in both NWT-subgroups (successful vs. failure) was comparable. Cause of NWT-failure was non-arousal (71%) or severe agitation (29%). Subjects with NWT failure subsequently had radiological examination (29%), repeat NWT (43%), continuous interruption of sedation (14%) or intracranial pressure (ICP) monitoring (14%). The primary reason for not doing NWTs was intracranial hypertension in 59%. Compared to the NWT-group, the non-NWT group had a higher PRISM III score (18.9 vs. 10.6), lower GCS/GMS at discharge, more associated trauma, and circulatory support. Nine patients (25%) died during their PICU admission, none of them had an NWT.
Conclusion: We observed limited use of NWTs in pediatric severe TBI. Patients who failed the NWT were indistinguishable from those without NWT. Both groups were more severely affected compared to the NWT successes. Therefore, our results may indicate that only a select group of severe pTBI patients qualify for the NWT.
Keywords: NWT; neurocritical care; pediatric; traumatic brain injury; wake-up test.
© 2024 Mulder, Helfferich and Kneyber.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The neurological wake-up test does not alter cerebral energy metabolism and oxygenation in patients with severe traumatic brain injury.Neurocrit Care. 2014 Jun;20(3):413-26. doi: 10.1007/s12028-013-9876-4. Neurocrit Care. 2014. PMID: 23934408
-
The Neurological Wake-up Test-A Role in Neurocritical Care Monitoring of Traumatic Brain Injury Patients?Front Neurol. 2017 Oct 17;8:540. doi: 10.3389/fneur.2017.00540. eCollection 2017. Front Neurol. 2017. PMID: 29089921 Free PMC article. Review.
-
Impact of Glasgow Coma Scale score and pupil parameters on mortality rate and outcome in pediatric and adult severe traumatic brain injury: a retrospective, multicenter cohort study.J Neurosurg. 2017 Mar;126(3):760-767. doi: 10.3171/2016.1.JNS152385. Epub 2016 Apr 1. J Neurosurg. 2017. PMID: 27035177
-
Analysis of long-term (median 10.5 years) outcomes in children presenting with traumatic brain injury and an initial Glasgow Coma Scale score of 3 or 4.J Neurosurg Pediatr. 2015 Oct;16(4):410-9. doi: 10.3171/2015.3.PEDS14679. Epub 2015 Jul 3. J Neurosurg Pediatr. 2015. PMID: 26140392
-
Neurologic Assessment of the Neurocritical Care Patient.Front Neurol. 2021 Mar 22;12:588989. doi: 10.3389/fneur.2021.588989. eCollection 2021. Front Neurol. 2021. PMID: 33828517 Free PMC article. Review.
Cited by
-
Early neurological wake-up test in intubated patients with traumatic brain injury.Int J Emerg Med. 2025 Mar 31;18(1):63. doi: 10.1186/s12245-025-00867-7. Int J Emerg Med. 2025. PMID: 40165068 Free PMC article.
References
-
- Kochanek PM, Tasker RC, Carney N, Totten MA, Adelson PD, Selden NR, et al. Guidelines for the management of pediatric severe traumatic brain injury, third edition: update of the brain trauma foundation guidelines. Pediatr Crit Care Med. (2019) 20(Suppl 1):S1–82. 10.1097/PCC.0000000000001735 - DOI - PubMed
-
- Shein SL, Ferguson NM, Kochanek PM, Bayir H, Clark RSB, Fink EL, et al. Effectiveness of pharmacological therapies for intracranial hypertension in children with severe traumatic brain injury–results from an automated data collection system time-synched to drug administration. Pediatr Crit Care Med. (2016) 17:236–45. 10.1097/PCC.0000000000000610 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous