

Subcutaneous anakinra in the management of refractory MIS-C in France
- PMID: 38464895
- PMCID: PMC10920278
- DOI: 10.3389/fped.2024.1270878
Subcutaneous anakinra in the management of refractory MIS-C in France
Abstract
Introduction: Multisystemic inflammatory syndrome in children (MIS-C) is a therapeutic emergency and can lead to myocardial dysfunction (17%-75%) and heart failure (52%-53%). Intravenous immunoglobulins (IVIG) and corticosteroids (CST) have been validated for the management of this condition. Recent reports suggest that an interleukin-1 (IL-1) receptor antagonist, namely anakinra, may be a valuable add-on to the 2019 novel coronavirus disease (COVID-19) treatment for refractory patients. The purpose of this study was to describe the clinico-biological characteristics of patients treated with anakinra as well as the efficacy and safety of subcutaneous anakinra therapy in this condition.
Methods: The prospective multicentre study of children hospitalized for MIS-C between March 2020 and September 2022, including 23 international paediatric centres, followed for a mean duration of 3.072 ± 3.508 months. The patient data were extracted from the Juvenile Inflammatory Rheumatism (JIR) cohort. The clinico-pathological characteristics, cardiac ultrasound data, and adverse events were reported in patients receiving anakinra.
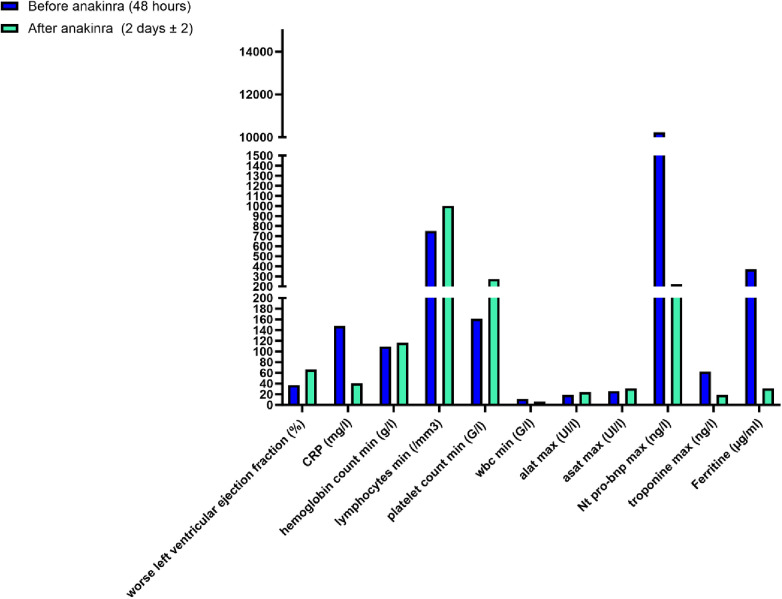
Results: Of the 470 children admitted with MIS-C, 18 French patients (50% girls) with a mean age of 10.06 ± 3.9 years were treated with subcutaneous anakinra. Anakinra was used in two situations, macrophage activation syndrome (MAS) (4 patients) and heart failure (14 patients) with a median left ventricular ejection fraction (LVEF) of 39.5% (30%-45%). The average dose of anakinra received was 2.53 ± 1.3 mg/kg/day for a median duration of 3 days. Prior to introduction, 78% (n = 14/18) of the patients had received CST and 56% (n = 10/18) had received IVIG. Only two patients received IVIG alone and six received CST alone plus anakinra. In 10% of cases, IVIG was poorly tolerated from a cardiovascular point of view and was discontinued. Transient elevations in serum transaminases were noted in four patients on anakinra without the need for treatment or dose modification. In all patients, rapid (48 h) improvement in myocardial function was observed (LVEF > 55%) with a concomitant significant decrease in myocardial enzymes (p < 0.05). All patients survived with complete recovery of cardiac function without sequelae.
Conclusions: Subcutaneous anakinra appears to be a safe and effective treatment for the management of heart failure or MAS in MIS-C patients. The value of IVIG in these two situations remains to be reviewed.
Keywords: COVID-19; anakinra; epidemiology; interleukin-1; multisystem inflammatory syndrome in children; myocarditis.
© 2024 Dusser, Belot, Bajolle, Kevorkian-Verguet, Meinzer, Huet, Tiriau and Kone-paut.
Conflict of interest statement
IK-p received honoraria as speaker or consultant from SOBI, Novartis, LFB, PFIZER, zydus, Cellgene, frezenius Kabi, CHUGAI but not for this work. PD received congress fees from SOBI, Novartis, Abbvie, PFIZER. AB reports consulting fees from Kabi, Roche Chugai, GlaxoSmithKline, AbbVie, Novartis. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- Davies P, Evans C, Kanthimathinathan HK, Lillie J, Brierley J, Waters G, et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health. (2020) 4(9):669–77. 10.1016/S2352-4642(20)30215-7 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources