

Clinical characteristics of 4,520 paediatric patients infected with the SARS-CoV-2 omicron variant, in Xi'an, China
- PMID: 38464898
- PMCID: PMC10920270
- DOI: 10.3389/fped.2024.1325562
Clinical characteristics of 4,520 paediatric patients infected with the SARS-CoV-2 omicron variant, in Xi'an, China
Abstract
Background and objective: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has broad tissue tropism and high transmission, which are likely to perpetuate the pandemic. The study aim to analyze the clinicopathogenic characteristics in paediatric patients.
Methods: In this single-centre study, we retrospectively included all confirmed cases infected by SARS-CoV-2 infection at Xi'an Children's Hospital, China, from 1 December to 31 December 2022. The demographic, clinical, laboratory, and radiological features of the patients were analysed.
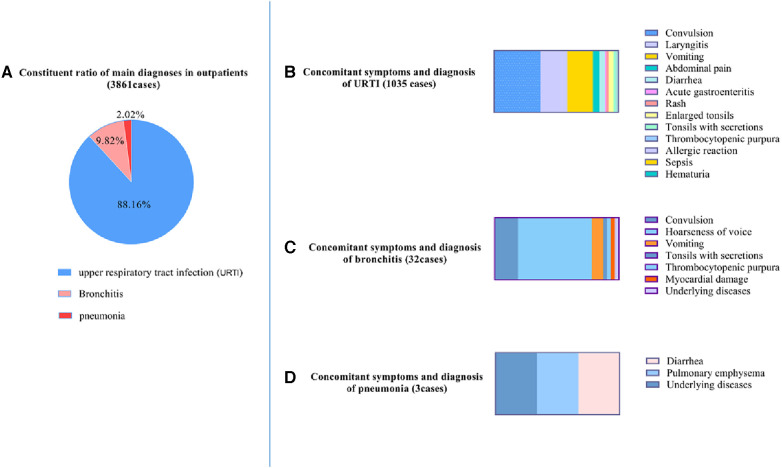
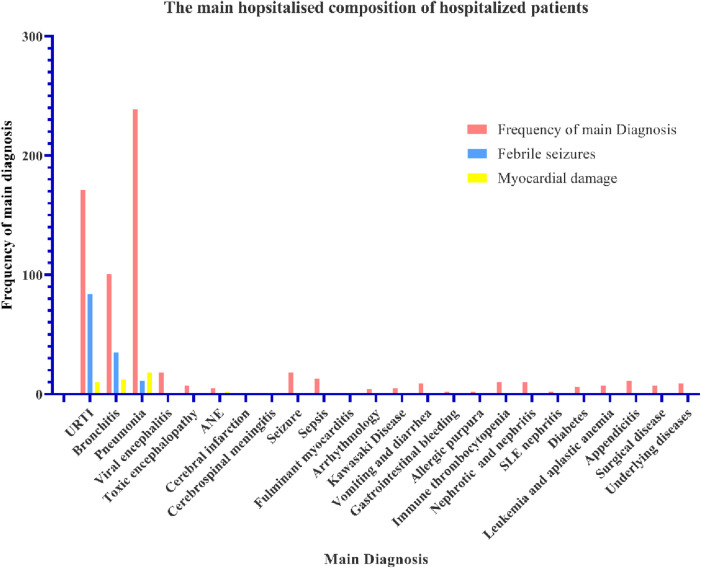
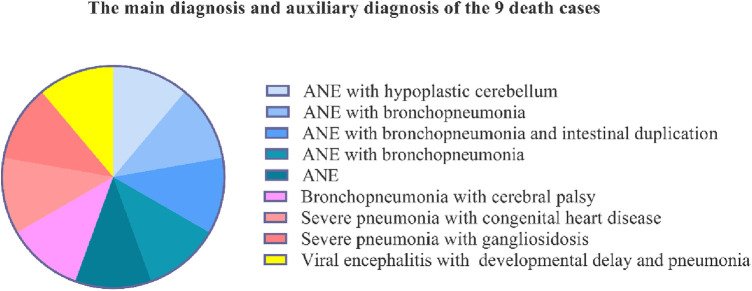
Results: A total of 4,520 paediatric patients with SARS-CoV-2 omicron variant infections were included. Of these, 3,861 (85.36%) were outpatients, 659 (14.64%) were hospitalised patients, and nine patients (0.20%) died. Of the nine patients who died, five were diagnosed with acute necrotising encephalopathy (ANE). The most common symptoms were fever in 4,275 (94.59%) patients, cough in 1,320 (29.20%) patients, convulsions in 610 (13.50%) patients, vomiting in 410 (9.07%) patients, runny nose/coryza in 277 (6.13%) patients, hoarseness of voice in 273 (6.04%) patients. A blood cell analysis showed a slight elevation of monocytes (mean: 11.14 ± 0.07%). The main diagnoses for both outpatients and inpatients were respiratory infection with multisystem manifestations.
Conclusions: A high incidence of convulsions is a typical characteristic of children infected with SARS-CoV-2. Five of the nine COVID-19 fatalities were associated with ANE. This indicates that nervous system damage in children with SARS-CoV-2 infection is more significant.
Keywords: COVID-19; SARS-CoV-2; acute necrotizing encephalopathy; coronavirus; omicron.
© 2024 Yue, Cao, Liu, Yin and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Acute necrotizing encephalopathy infected with the SARS-CoV-2 in children: Case series and literature review of clinical outcomes with the use of Tocilizumab.Eur J Paediatr Neurol. 2024 Sep;52:67-75. doi: 10.1016/j.ejpn.2024.07.009. Epub 2024 Jul 19. Eur J Paediatr Neurol. 2024. PMID: 39106789 Review.
-
[Clinical and imaging analysis of neurological complications in critically ill children infected with SARS-CoV-2 Omicron].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Nov;35(11):1157-1163. doi: 10.3760/cma.j.cn121430-20230117-00031. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37987125 Chinese.
-
Clinical characteristics and risk factors of severe COVID-19 in hospitalized neonates with omicron variant infection: a retrospective study.Ital J Pediatr. 2024 Sep 16;50(1):176. doi: 10.1186/s13052-024-01751-5. Ital J Pediatr. 2024. PMID: 39278913 Free PMC article.
-
Clinical characteristics of 1139 mild cases of the SARS-CoV-2 Omicron variant infected patients in Shanghai.J Med Virol. 2023 Jan;95(1):e28224. doi: 10.1002/jmv.28224. Epub 2022 Oct 26. J Med Virol. 2023. PMID: 36238984 Free PMC article.
-
Human and novel coronavirus infections in children: a review.Paediatr Int Child Health. 2021 Feb;41(1):36-55. doi: 10.1080/20469047.2020.1781356. Epub 2020 Jun 25. Paediatr Int Child Health. 2021. PMID: 32584199 Review.
Cited by
-
Clinical feature of omicron infection in children with inborn errors of immunity in China.Front Immunol. 2024 Jul 23;15:1420547. doi: 10.3389/fimmu.2024.1420547. eCollection 2024. Front Immunol. 2024. PMID: 39108271 Free PMC article.
-
Critically ill children with SARS-COV-2 Omicron infection at a national children medical center, Guangdong, China.BMC Pediatr. 2024 Apr 15;24(1):254. doi: 10.1186/s12887-024-04735-w. BMC Pediatr. 2024. PMID: 38622552 Free PMC article.
References
-
- World Health Organization. Classification of omicron (B.1.1.529): SARS-CoV-2 variant of concern. Updated 2021. (accessed December 22, 2021)).
LinkOut - more resources
Full Text Sources
Miscellaneous