

Development of an Algorithm to Screen for Frailty Using the Clinical Frailty Scale with Postoperative Patients Entering Cardiac Rehabilitation
- PMID: 38465304
- PMCID: PMC10919360
- DOI: 10.3138/ptc-2021-0098
Development of an Algorithm to Screen for Frailty Using the Clinical Frailty Scale with Postoperative Patients Entering Cardiac Rehabilitation
Abstract
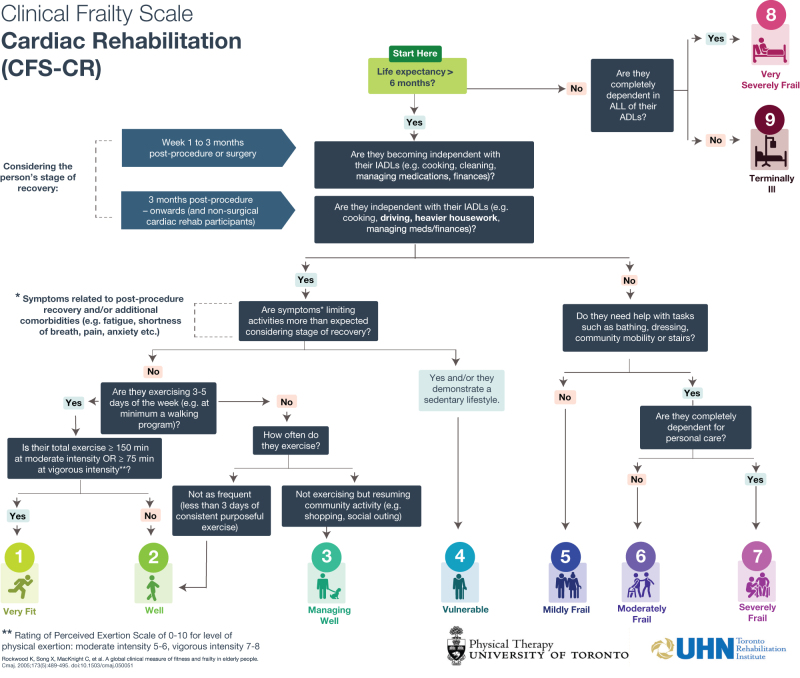
Purpose: Frailty is not commonly assessed on intake to cardiac rehabilitation (CR), but screening could enable targeted interventions and potentially reduce secondary complications. This study aimed to develop and retrospectively examine the feasibility of utilizing a CR-specific algorithm based on the Clinical Frailty Scale (CFS). Our CFS-CR algorithm endeavoured to screen for frailty in older adults (> 65 y) entering CR following cardiac surgery/procedure.
Method: The charts of 30 former patients (mean age: 74.0 ± 6.9 y) were examined by a clinician working in CR.
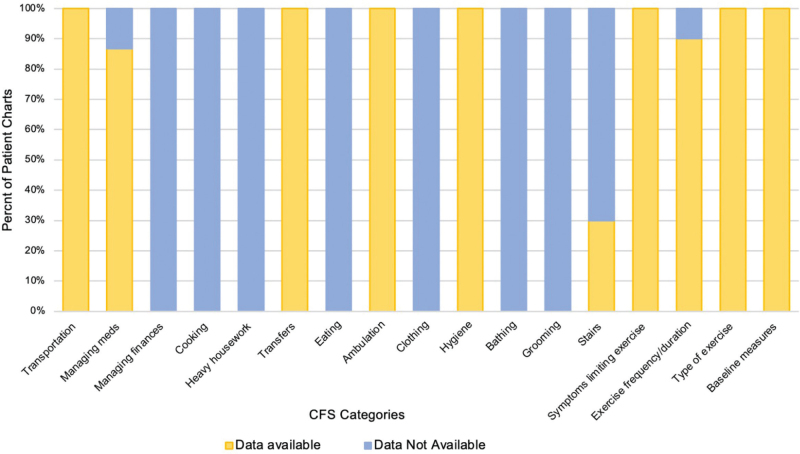
Results: The clinician was unable to score any of the patients based on their medical charts using the CFS-CR due to insufficient data. Documentation was typically limited in the areas of instrumental and basic activities of daily living whereas exercise data were readily available.
Conclusions: Current intake documentation in CR limited the ability to retrospectively screen for frailty. This finding suggests a need for a frailty-specific tool to support routine clinical screening. Prospective evaluation of the CFS-CR is warranted to further examine the clinical utility of the algorithm during CR intake assessments.
Objectif: la fragilité est peu évaluée à l’admission en réadaptation cardiaque (RC), mais le dépistage pourrait permettre de cibler des interventions et peutêtre de réduire les complications secondaires. La présente étude visait à créer un algorithme de RC d’après l’échelle de fragilité clinique (ÉFC) et à procéder à une analyse rétrospective pour déterminer la faisabilité de l’utiliser. L’algorithme ÉFC-RC était conçu pour dépister la fragilité chez les personnes âgées (de 65 ans ou plus) qui arrivaient en RC après une opération ou une intervention cardiaque.
Méthodologie: une clinicienne qui travaillait en RC a examiné les dossiers de 30 anciens patients (âge moyen de 74,0 ± 6,9 ans).
Résultats: la clinicienne n’a pu mesurer les résultats d’aucun patient d’après leur dossier médical au moyen de l’ÉFC-RC en raison de données insuffisantes. Les éléments du dossier se limitaient généralement aux activités déterminantes et courantes de la vie quotidienne, tandis que les données sur les exercices étaient facilement accessibles.
Conclusions: l’information contenue dans les dossiers d’admission actuels en RC limitait la possibilité de procéder à l’analyse rétrospective de la fragilité. Cette observation laisse croire à la nécessité de concevoir un outil axé sur la fragilité pour contribuer au dépistage clinique systématique. Une évaluation prospective de l’ÉFC-RC s’impose pour mieux analyser l’utilité clinique de l’algorithme lors des évaluations à l’admission en RC.
Keywords: adult; algorithms; cardiac rehabilitation; frailty; geriatric assessment.
© Canadian Physiotherapy Association, 2024.
Conflict of interest statement
Competing Interests: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Evaluation of frailty in geriatric patients undergoing cardiac rehabilitation after cardiac procedure: results of a prospective, cross-sectional study.BMC Sports Sci Med Rehabil. 2024 Jul 2;16(1):146. doi: 10.1186/s13102-024-00937-y. BMC Sports Sci Med Rehabil. 2024. PMID: 38956610 Free PMC article.
-
Inter-Rater Reliability of the Retrospectively Assigned Clinical Frailty Scale Score in a Geriatric Outreach Population.Can Geriatr J. 2018 Mar 26;21(1):1-5. doi: 10.5770/cgj.21.263. eCollection 2018 Mar. Can Geriatr J. 2018. PMID: 29581815 Free PMC article.
-
Clinical frailty scale score during geriatric rehabilitation predicts short-term mortality: RESORT cohort study.Ann Phys Rehabil Med. 2023 Feb;66(1):101645. doi: 10.1016/j.rehab.2022.101645. Epub 2022 Dec 1. Ann Phys Rehabil Med. 2023. PMID: 35151896
-
Frailty and Exercise Training: How to Provide Best Care after Cardiac Surgery or Intervention for Elder Patients with Valvular Heart Disease.Biomed Res Int. 2018 Sep 13;2018:9849475. doi: 10.1155/2018/9849475. eCollection 2018. Biomed Res Int. 2018. PMID: 30302342 Free PMC article. Review.
-
Cardiac rehabilitation and frailty: a systematic review and meta-analysis.Eur J Prev Cardiol. 2024 Nov 18;31(16):1960-1976. doi: 10.1093/eurjpc/zwae239. Eur J Prev Cardiol. 2024. PMID: 39036978
References
LinkOut - more resources
Full Text Sources