

Lung microbiota composition, respiratory mechanics, and outcomes in COVID-19-related ARDS
- PMID: 38466118
- PMCID: PMC10986322
- DOI: 10.1128/spectrum.03574-23
Lung microbiota composition, respiratory mechanics, and outcomes in COVID-19-related ARDS
Abstract
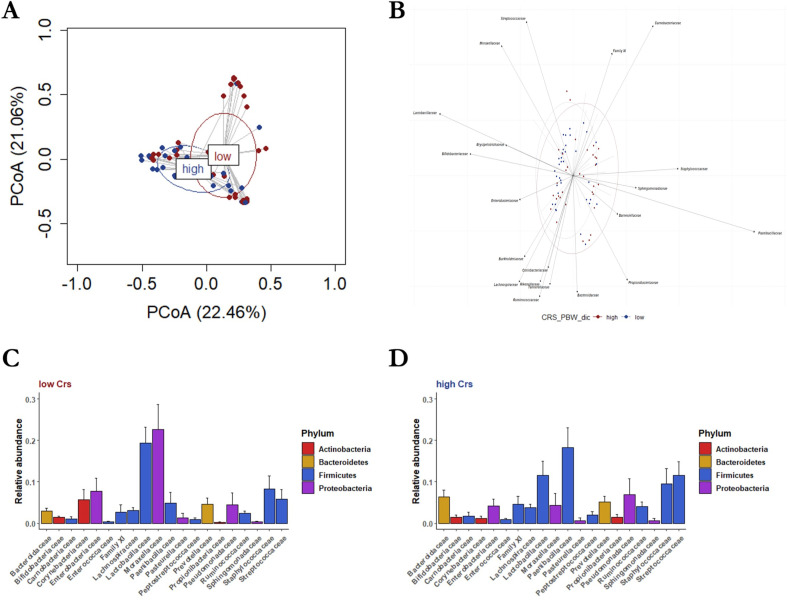
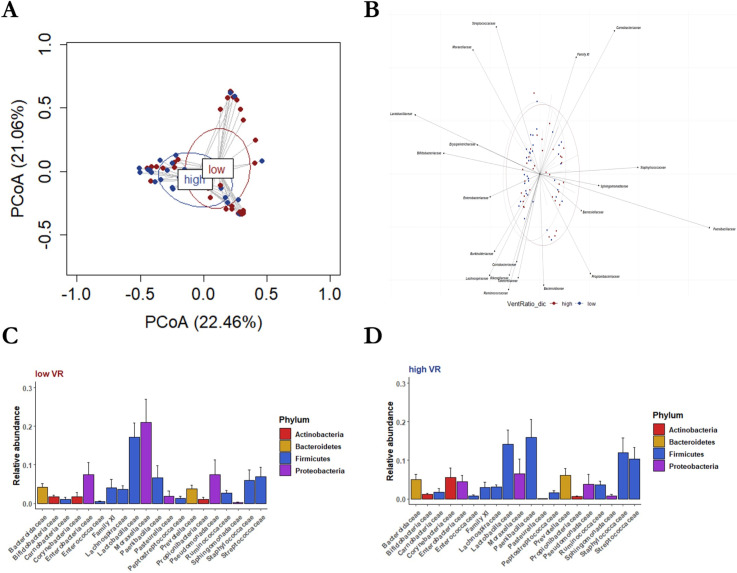
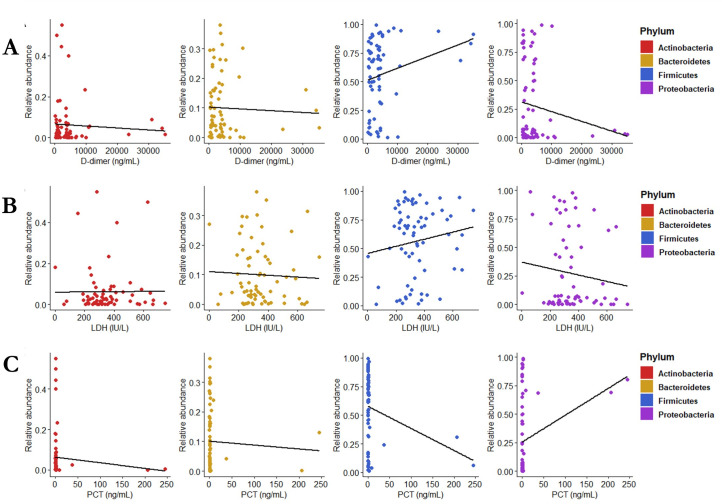
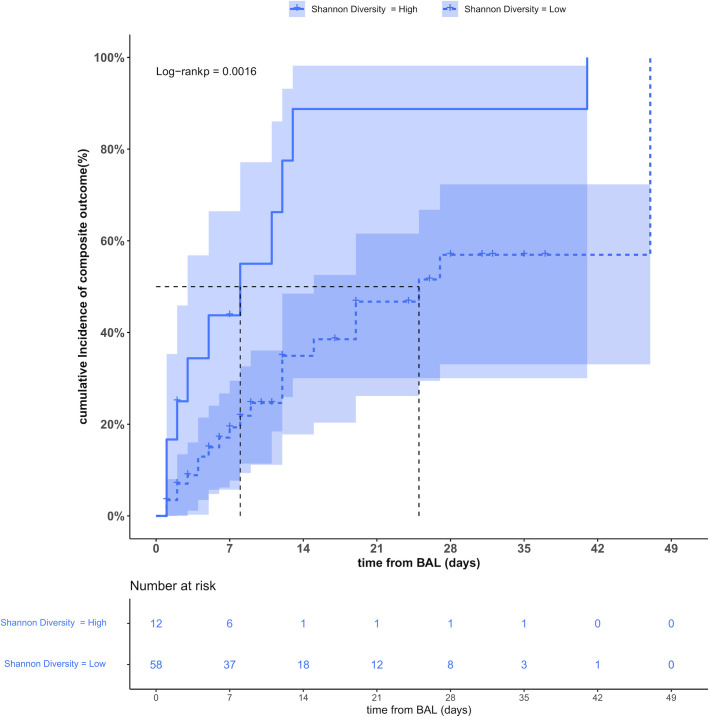
Few data are available on the lung microbiota composition of patients with coronavirus disease 2019-related acute respiratory distress syndrome (C-ARDS) receiving invasive mechanical ventilation (IMV). Moreover, it has never been investigated whether there is a potential correlation between lung microbiota communities and respiratory mechanics. We performed a prospective observational study in two intensive care units of a university hospital in Italy. Lung microbiota was investigated by bacterial 16S rRNA gene sequencing, performed on bronchoalveolar lavage fluid samples withdrawn after intubation. The lung bacterial communities were analyzed after stratification by respiratory system compliance/predicted body weight (Crs) and ventilatory ratio (VR). Weaning from IMV and hospital survival were assessed as secondary outcomes. In 70 C-ARDS patients requiring IMV from 1 April through 31 December 2020, the lung microbiota composition (phylum taxonomic level, permutational multivariate analysis of variance test) significantly differed between who had low Crs vs those with high Crs (P = 0.010), as well as in patients with low VR vs high VR (P = 0.012). As difference-driving taxa, Proteobacteria (P = 0.017) were more dominant and Firmicutes (P = 0.040) were less dominant in low- vs high-Crs patients. Similarly, Proteobacteria were more dominant in low- vs high-VR patients (P = 0.013). After multivariable regression analysis, we further observed lung microbiota diversity as a negative predictor of weaning from IMV and hospital survival (hazard ratio = 3.31; 95% confidence interval, 1.52-7.20, P = 0.048). C-ARDS patients with low Crs/low VR had a Proteobacteria-dominated lung microbiota. Whether patients with a more diverse lung bacterial community may have more chances to be weaned from IMV and discharged alive from the hospital warrants further large-scale investigations.
Importance: Lung microbiota characteristics were demonstrated to predict ventilator-free days and weaning from mechanical ventilation in patients with acute respiratory distress syndrome (ARDS). In this study, we observed that in severe coronavirus disease 2019 patients with ARDS who require invasive mechanical ventilation, lung microbiota characteristics were associated with respiratory mechanics. Specifically, the lung microbiota of patients with low respiratory system compliance and low ventilatory ratio was characterized by Proteobacteria dominance. Moreover, after multivariable regression analysis, we also found an association between patients' microbiota diversity and a higher possibility of being weaned from mechanical ventilation and discharged alive from the hospital. For these reasons, lung microbiota characterization may help to stratify patient characteristics and orient the delivery of target interventions. (This study has been registered at ClinicalTrials.gov on 17 February 2020 under identifier NCT04271345.).
Registered at ClinicalTrials.gov, 17 February 2020 (NCT0427135).
Keywords: ARDS; COVID-19; microbiota; mortality; respiratory mechanics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Positioning for acute respiratory distress in hospitalised infants and children.Cochrane Database Syst Rev. 2022 Jun 6;6(6):CD003645. doi: 10.1002/14651858.CD003645.pub4. Cochrane Database Syst Rev. 2022. PMID: 35661343 Free PMC article.
-
Ventilator Management(Archived).2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28846232 Free Books & Documents.
-
Partial liquid ventilation for preventing death and morbidity in adults with acute lung injury and acute respiratory distress syndrome.Cochrane Database Syst Rev. 2013 Jul 23;2013(7):CD003707. doi: 10.1002/14651858.CD003707.pub3. Cochrane Database Syst Rev. 2013. PMID: 23881653 Free PMC article.
-
SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19.Cochrane Database Syst Rev. 2021 Sep 2;9(9):CD013825. doi: 10.1002/14651858.CD013825.pub2. Cochrane Database Syst Rev. 2021. PMID: 34473343 Free PMC article.
-
Early spontaneous breathing for acute respiratory distress syndrome in individuals with COVID-19.Cochrane Database Syst Rev. 2022 Jun 29;6(6):CD015077. doi: 10.1002/14651858.CD015077. Cochrane Database Syst Rev. 2022. PMID: 35767435 Free PMC article.
Cited by
-
Impact of Invasive Mechanical Ventilation on the Lung Microbiome.Adv Respir Med. 2025 Jul 1;93(4):23. doi: 10.3390/arm93040023. Adv Respir Med. 2025. PMID: 40700054 Free PMC article. Review.
-
Lung microbiota: a new hope for treating acute respiratory distress syndrome?Front Microbiol. 2025 May 30;16:1586949. doi: 10.3389/fmicb.2025.1586949. eCollection 2025. Front Microbiol. 2025. PMID: 40520382 Free PMC article. Review.
-
Impact of fecal microbiota transplantation on lung function and gut microbiome in an ARDS rat model: A multi-omics analysis including 16S rRNA sequencing, metabolomics, and transcriptomics.Int J Immunopathol Pharmacol. 2025 Jan-Dec;39:3946320251333982. doi: 10.1177/03946320251333982. Epub 2025 Apr 23. Int J Immunopathol Pharmacol. 2025. PMID: 40265594 Free PMC article.
-
Mechanisms by Which the Intratumoral Microbiome May Potentiate Immunotherapy Response.J Clin Oncol. 2024 Oct;42(28):3350-3352. doi: 10.1200/JCO.24.00908. Epub 2024 Jul 26. J Clin Oncol. 2024. PMID: 39058969 No abstract available.
References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, LUNG SAFE Investigators, ESICM Trials Group . 2016. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 315:788–800. doi:10.1001/jama.2016.0291 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
