

Tumor-Infiltrating Lymphocytes Refine Outcomes in Triple-Negative Breast Cancer Treated with Anthracycline-Free Neoadjuvant Chemotherapy
- PMID: 38466643
- PMCID: PMC11096004
- DOI: 10.1158/1078-0432.CCR-24-0106
Tumor-Infiltrating Lymphocytes Refine Outcomes in Triple-Negative Breast Cancer Treated with Anthracycline-Free Neoadjuvant Chemotherapy
Abstract
Purpose: Stromal tumor-infiltrating lymphocytes (sTIL) are associated with pathologic complete response (pCR) and long-term outcomes for triple-negative breast cancer (TNBC) in the setting of anthracycline-based chemotherapy. The impact of sTILs on refining outcomes beyond prognostic information provided by pCR in anthracycline-free neoadjuvant chemotherapy (NAC) is not known.
Experimental design: This is a pooled analysis of two studies where patients with stage I (T>1 cm)-III TNBC received carboplatin (AUC 6) plus docetaxel (75 mg/m2; CbD) NAC. sTILs were evaluated centrally on pre-treatment hematoxylin and eosin slides using standard criteria. Cox regression analysis was used to examine the effect of variables on event-free survival (EFS) and overall survival (OS).
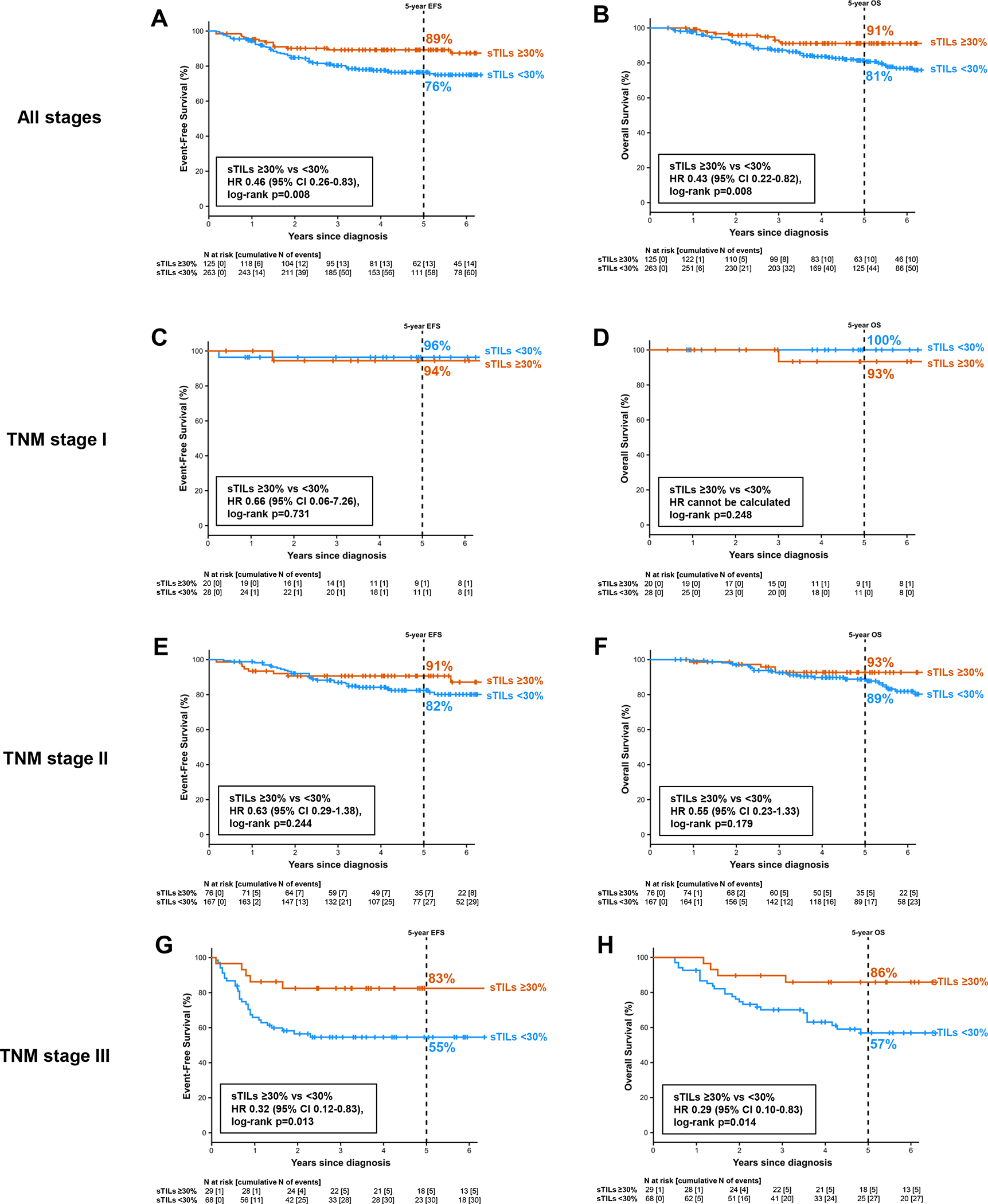
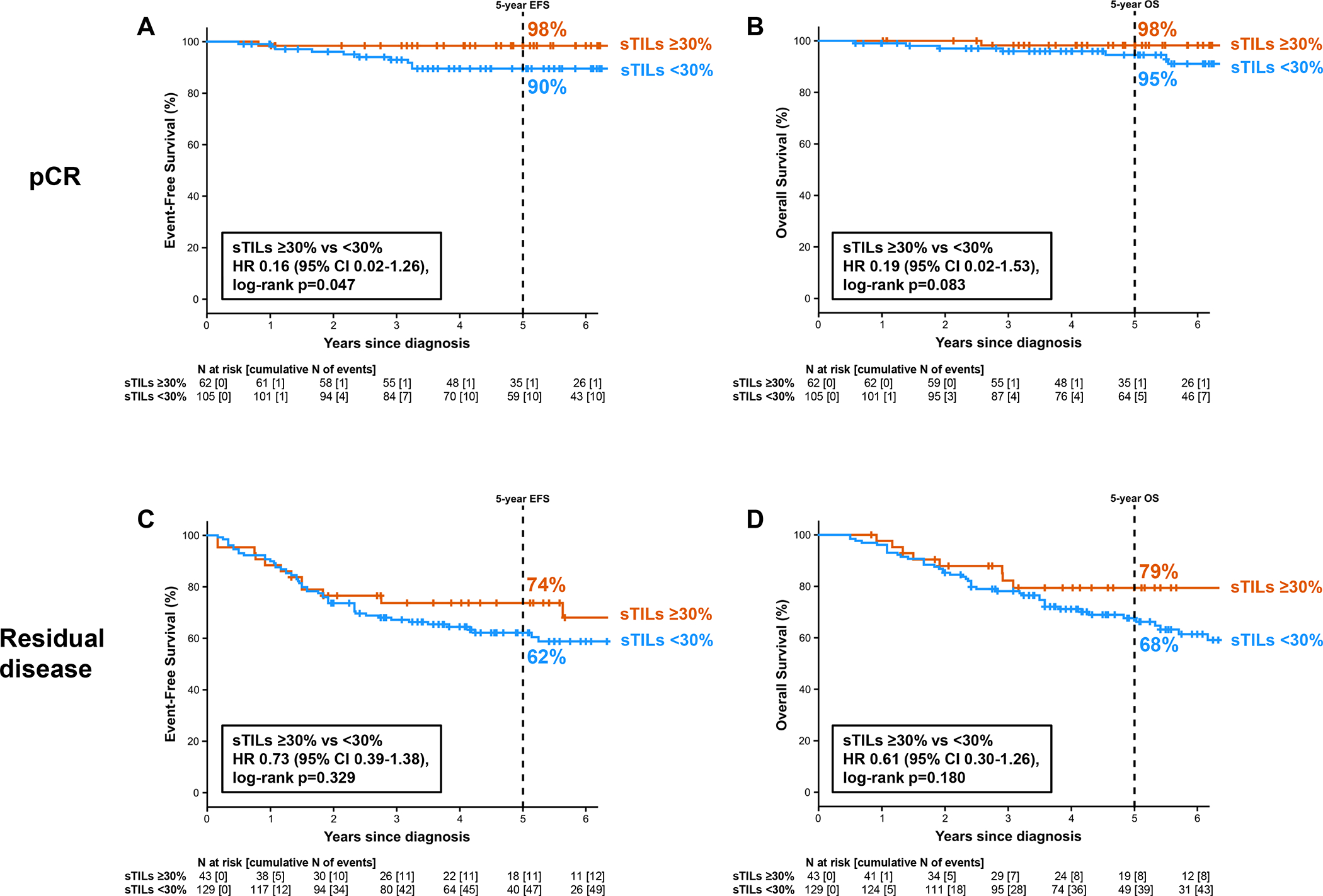
Results: Among 474 patients, 44% had node-positive disease. Median sTILs were 5% (range, 1%-95%), and 32% of patients had ≥30% sTILs. pCR rate was 51%. On multivariable analysis, T stage (OR, 2.08; P = 0.007), nodal status (OR, 1.64; P = 0.035), and sTILs (OR, 1.10; P = 0.011) were associated with pCR. On multivariate analysis, nodal status (HR, 0.46; P = 0.008), pCR (HR, 0.20; P < 0.001), and sTILs (HR, 0.95; P = 0.049) were associated with OS. At 30% cut-point, sTILs stratified outcomes in stage III disease, with 5-year OS 86% versus 57% in ≥30% versus <30% sTILs (HR, 0.29; P = 0.014), and numeric trend in stage II, with 5-year OS 93% versus 89% in ≥30% versus <30% sTILs (HR, 0.55; P = 0.179). Among stage II-III patients with pCR, EFS was better in those with ≥30% sTILs (HR, 0.16; P, 0.047).
Conclusions: sTILs density was an independent predictor of OS beyond clinicopathologic features and pathologic response in patients with TNBC treated with anthracycline-free CbD chemotherapy. Notably, sTILs density stratified outcomes beyond tumor-node-metastasis (TNM) stage and pathologic response. These findings highlight the role of sTILs in patient selection and stratification for neo/adjuvant escalation and de-escalation strategies.
©2024 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer. Version 4.2023. 2023. March 23, 2023. https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
