

U-shaped association between serum calcium and in-hospital mortality in patients with congestive heart failure
- PMID: 38467491
- PMCID: PMC11424285
- DOI: 10.1002/ehf2.14730
U-shaped association between serum calcium and in-hospital mortality in patients with congestive heart failure
Abstract
Aims: Serum calcium level is widely used for evaluating disease severity, but its impact on clinical outcomes in patients with congestive heart failure (CHF) remains poorly understood. The aim of this study is to investigate the relationship between serum calcium levels and in-hospital mortality in CHF patients.
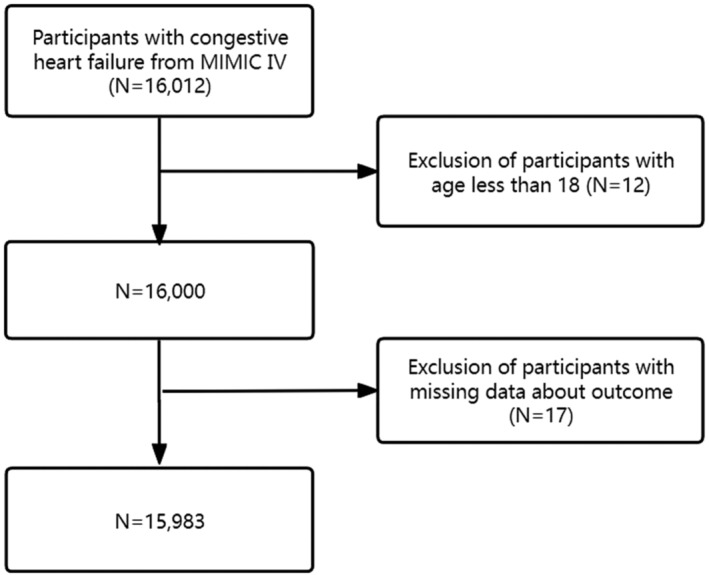
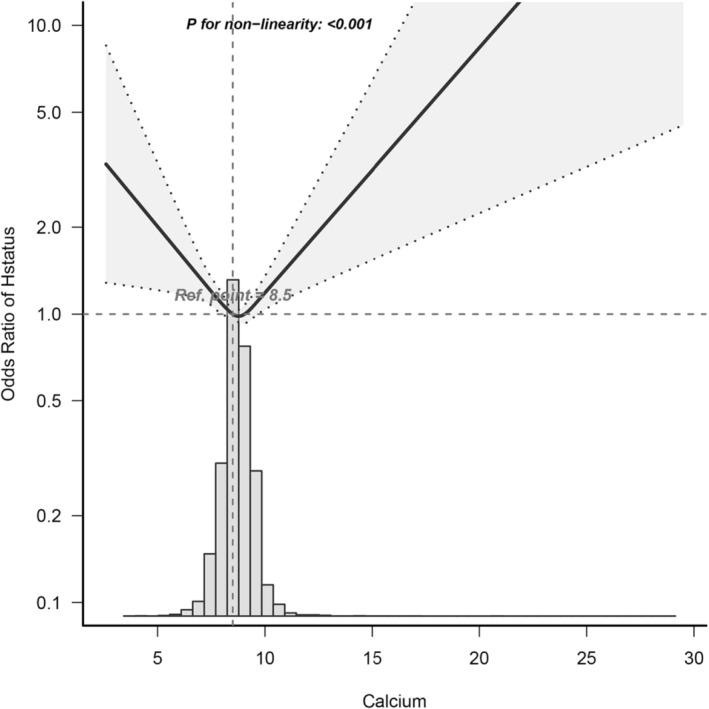
Methods and results: We conducted a retrospective analysis utilizing clinical data from the Medical Information Mart for Intensive Care database, encompassing a cohort of 15 983 CHF patients. This cohort was stratified based on their serum calcium levels, with the primary objective being the determination of in-hospital mortality. To assess the impact of admission serum calcium levels on in-hospital mortality, we employed various statistical methodologies, including multivariable logistic regression models, a generalized additive model, a two-piecewise linear regression model, and subgroup analysis. Comparative analysis of the reference group (Q3) revealed increased in-hospital mortality in the first quintile (Q1, the group with the lowest blood calcium level) and the fifth quintile (Q5, the group with the highest blood calcium level), with fully adjusted odds ratios of 1.38 [95% confidence interval (CI): 1.13-1.68, P = 0.002] and 1.23 (95% CI: 1.01-1.5, P = 0.038), respectively. A U-shaped relationship was observed between serum calcium levels and in-hospital mortality, with the lowest risk occurring at a threshold of 8.35 mg/dL. The effect sizes and corresponding CIs below and above this threshold were 0.782 (95% CI: 0.667-0.915, P = 0.0023) and 1.147 (95% CI: 1.034-1.273, P = 0.0094), respectively. Stratified analyses confirmed the robustness of this correlation.
Conclusions: Our study identifies a U-shaped association between serum calcium levels and in-hospital mortality in CHF patients, with a notable inflection point at 8.35 mg/dL. Further investigation through prospective, randomized, and controlled studies is warranted to validate the findings presented in this study.
Keywords: Association; Blood calcium; Congestive heart failure; Generalized additive model; In‐hospital mortality; Subgroup analysis.
© 2024 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
U-shaped association between serum calcium and in-hospital mortality in diabetes patients with congestive heart failure: a cohort study.Sci Rep. 2024 Jun 11;14(1):13412. doi: 10.1038/s41598-024-63603-w. Sci Rep. 2024. PMID: 38862553 Free PMC article.
-
U-Shaped Association between Serum Chloride Levels and In-Hospital Mortality in Patients with Congestive Heart Failure in Intensive Care Units.Int Heart J. 2024;65(2):237-245. doi: 10.1536/ihj.23-331. Int Heart J. 2024. PMID: 38556334
-
Association Between Body Temperature and In-Hospital Mortality Among Congestive Heart Failure Patients with Diabetes in Intensive Care Unit: A Retrospective Cohort Study.Ther Hypothermia Temp Manag. 2024 Sep;14(3):197-204. doi: 10.1089/ther.2023.0053. Epub 2023 Nov 15. Ther Hypothermia Temp Manag. 2024. PMID: 37971393
-
Association Between Systolic Blood Pressure and in-Hospital Mortality Among Congestive Heart Failure Patients with Chronic Obstructive Pulmonary Disease in the Intensive Care Unit: A Retrospective Cohort Study.Int J Chron Obstruct Pulmon Dis. 2024 Sep 13;19:2023-2034. doi: 10.2147/COPD.S448332. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39291240 Free PMC article.
-
The relationship between serum anion gap levels and short-, medium-, and long-term all-cause mortality in ICU patients with congestive heart failure: a retrospective cohort study.Acta Cardiol. 2024 Aug;79(6):705-719. doi: 10.1080/00015385.2024.2371627. Epub 2024 Jul 2. Acta Cardiol. 2024. PMID: 38953283
Cited by
-
Association between admission serum calcium levels and in‑hospital mortality in acute myocardial infarction patients with cardiovascular-kidney-metabolic syndrome.Endocrine. 2025 Jul;89(1):232-239. doi: 10.1007/s12020-025-04217-8. Epub 2025 Mar 29. Endocrine. 2025. PMID: 40156686 Free PMC article.
References
-
- Tang Y, Chen Q, Liang B, Peng B, Wang M, Sun J, et al. A retrospective cohort study on the association between early coagulation disorder and short‐term all‐cause mortality of critically ill patients with congestive heart failure. Front Cardiovasc Med 2022;9:999391. doi:10.3389/fcvm.2022.999391 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
