

Impact of vaccination on the association of COVID-19 with cardiovascular diseases: An OpenSAFELY cohort study
- PMID: 38467603
- PMCID: PMC10928172
- DOI: 10.1038/s41467-024-46497-0
Impact of vaccination on the association of COVID-19 with cardiovascular diseases: An OpenSAFELY cohort study
Abstract
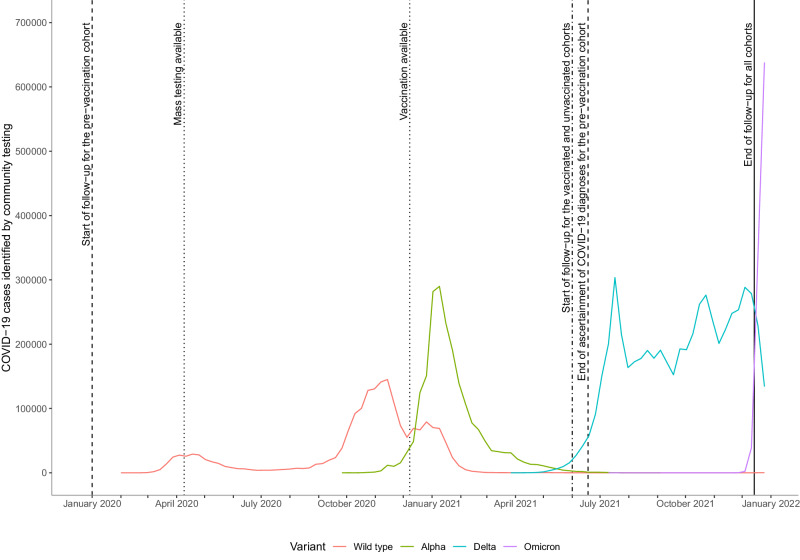
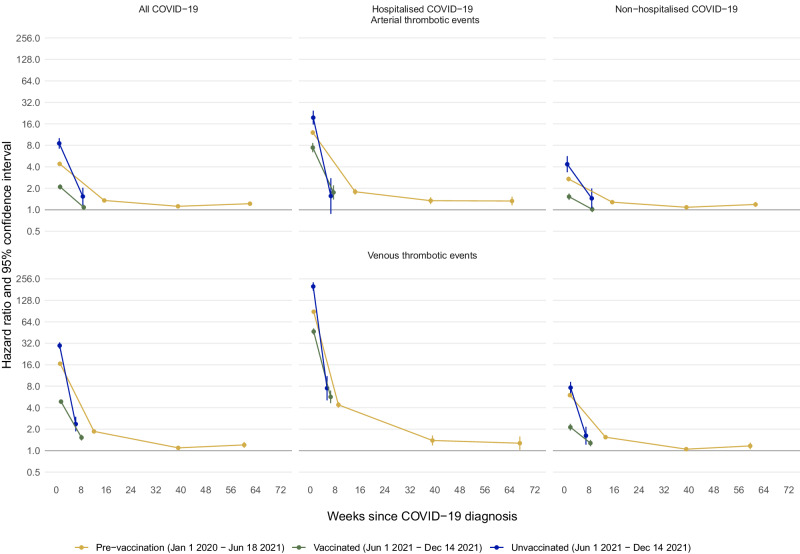
Infection with SARS-CoV-2 is associated with an increased risk of arterial and venous thrombotic events, but the implications of vaccination for this increased risk are uncertain. With the approval of NHS England, we quantified associations between COVID-19 diagnosis and cardiovascular diseases in different vaccination and variant eras using linked electronic health records for ~40% of the English population. We defined a 'pre-vaccination' cohort (18,210,937 people) in the wild-type/Alpha variant eras (January 2020-June 2021), and 'vaccinated' and 'unvaccinated' cohorts (13,572,399 and 3,161,485 people respectively) in the Delta variant era (June-December 2021). We showed that the incidence of each arterial thrombotic, venous thrombotic and other cardiovascular outcomes was substantially elevated during weeks 1-4 after COVID-19, compared with before or without COVID-19, but less markedly elevated in time periods beyond week 4. Hazard ratios were higher after hospitalised than non-hospitalised COVID-19 and higher in the pre-vaccination and unvaccinated cohorts than the vaccinated cohort. COVID-19 vaccination reduces the risk of cardiovascular events after COVID-19 infection. People who had COVID-19 before or without being vaccinated are at higher risk of cardiovascular events for at least two years.
© 2024. The Author(s).
Conflict of interest statement
WW is supported by the Chief Scientist’s Office, the Stroke Association, and the Alzheimer’s Society; sits on data monitoring committees for academic trials (TEMPO-2, PROTECT-U, and CATIS-ICAD); and is an independent expert witness to UK courts. NC receives funds from AstraZeneca to support membership of Data Safety and Monitoring Committees for clinical trials. CH is the Principal Investigator of a study which is a collaboration sponsored by the University of Bristol and funded by Pfizer Inc. The other authors report no conflicts.
Figures


References
-
- Campbell, F. et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Eurosurveillance. 2021;26. Available from: https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2021.26.24.... - DOI - PMC - PubMed
-
- World Health Organisation. Weekly epidemiological update on COVID-19 - 20 July 2021. 2021. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on...
-
- Public Health England. SARS-CoV-2 variants of concern and variants under investigation: technical briefing 14. 2021. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploa...
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
