Cognitive profile in cerebral small vessel disease: comparison between cerebral amyloid angiopathy and hypertension-related microangiopathy
- PMID: 38467658
- PMCID: PMC10928167
- DOI: 10.1038/s41598-024-55719-w
Cognitive profile in cerebral small vessel disease: comparison between cerebral amyloid angiopathy and hypertension-related microangiopathy
Erratum in
-
Author Correction: Cognitive profile in cerebral small vessel disease: comparison between cerebral amyloid angiopathy and hypertension-related microangiopathy.Sci Rep. 2024 Apr 16;14(1):8792. doi: 10.1038/s41598-024-59216-y. Sci Rep. 2024. PMID: 38627411 Free PMC article. No abstract available.
Abstract
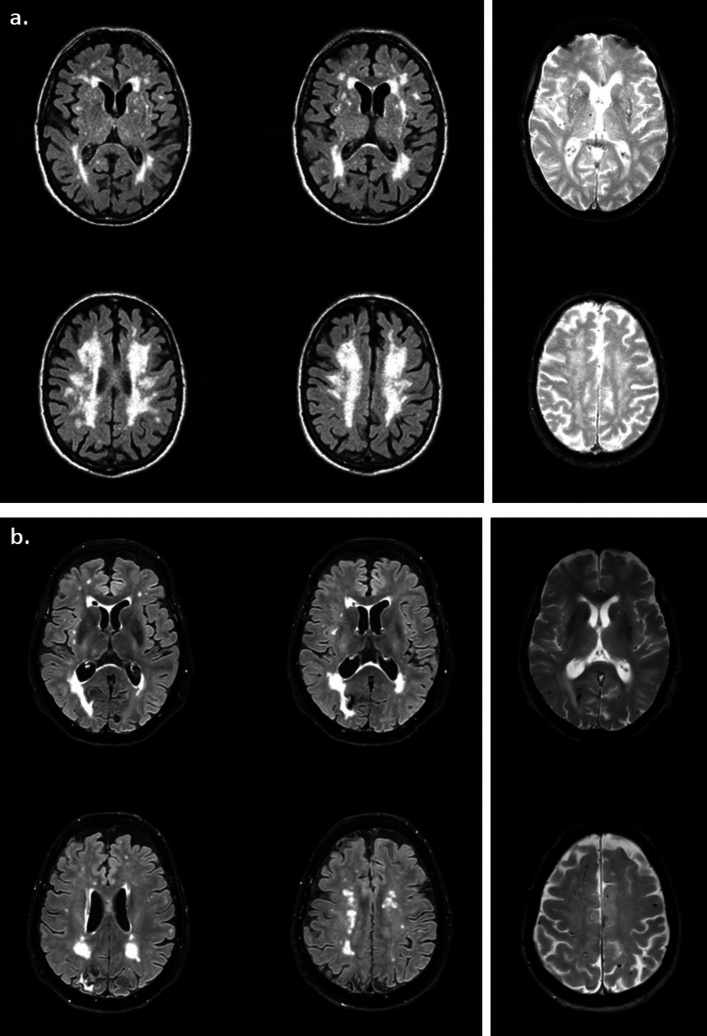
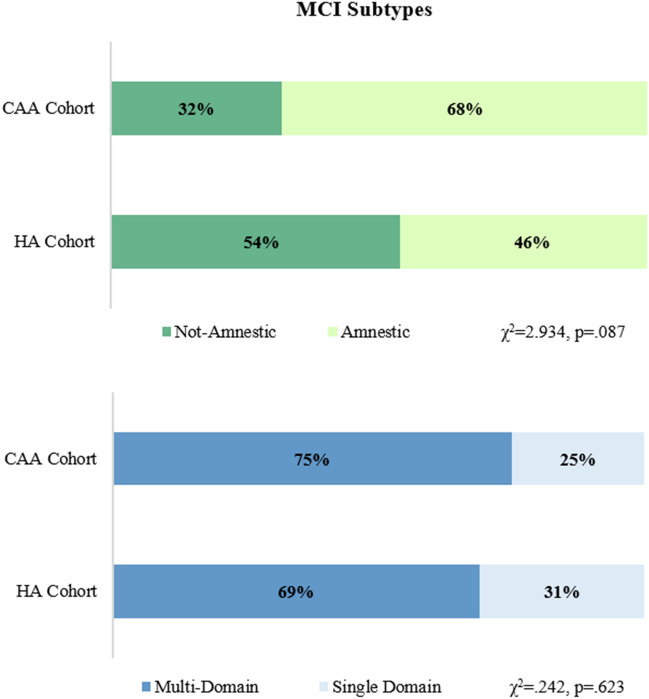
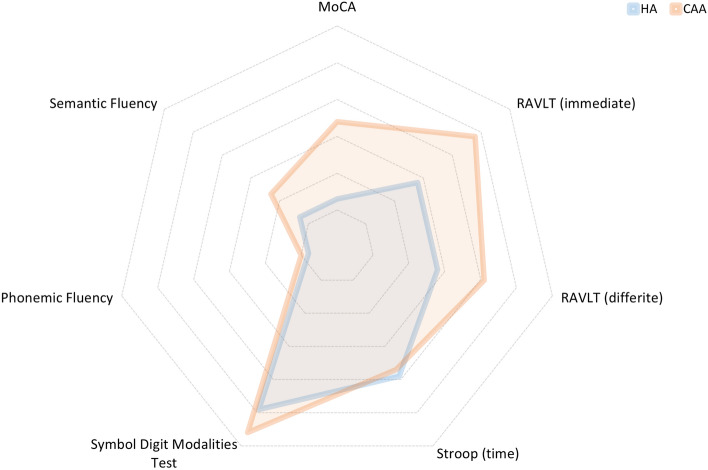
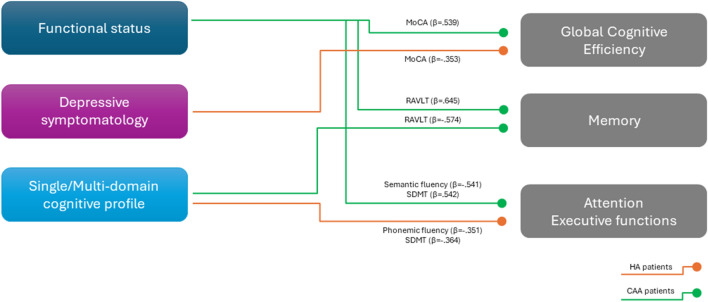
Cerebral amyloid angiopathy (CAA) is recognized as a cause of cognitive impairment, but its cognitive profile needs to be characterized, also respect to hypertension-related microangiopathy (HA). We aimed at comparing difference or similarity of CAA and HA patients' cognitive profiles, and their associated factors. Participants underwent an extensive clinical, neuropsychological, and neuroimaging protocol. HA patients (n = 39) were more frequently males, with history of vascular risk factors than CAA (n = 32). Compared to HA, CAA patients presented worse performance at MoCA (p = 0.001) and semantic fluency (p = 0.043), and a higher prevalence of amnestic MCI (46% vs. 68%). In univariate analyses, multi-domain MCI was associated with worse performance at MoCA, Rey Auditory Verbal Learning Test (RAVLT), and semantic fluency in CAA patients, and with worse performance at Symbol Digit Modalities Test (SDMT) and phonemic fluency in HA ones. In multivariate models, multi-domain deficit remained as the only factor associated with RAVLT (β = - 0.574) in CAA, while with SDMT (β = - 0.364) and phonemic fluency (β = - 0.351) in HA. Our results highlight different patterns of cognitive deficits in CAA or HA patients. While HA patients' cognitive profile was confirmed as mainly attentional/executive, a complex cognitive profile, characterized also by deficit in semantic memory, seems the hallmark of CAA patients.
Keywords: Arteriolosclerosis; Cerebral amyloid angiopathy; Cerebral small vessel disease; Cognition; Cognitive decline; Cognitive impairment; Cognitive profile; Microangiopathy; Neuropsychological patterns.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures