

Comprehensive proteomics of CSF, plasma, and urine identify DDC and other biomarkers of early Parkinson's disease
- PMID: 38467937
- PMCID: PMC10927779
- DOI: 10.1007/s00401-024-02706-0
Comprehensive proteomics of CSF, plasma, and urine identify DDC and other biomarkers of early Parkinson's disease
Abstract
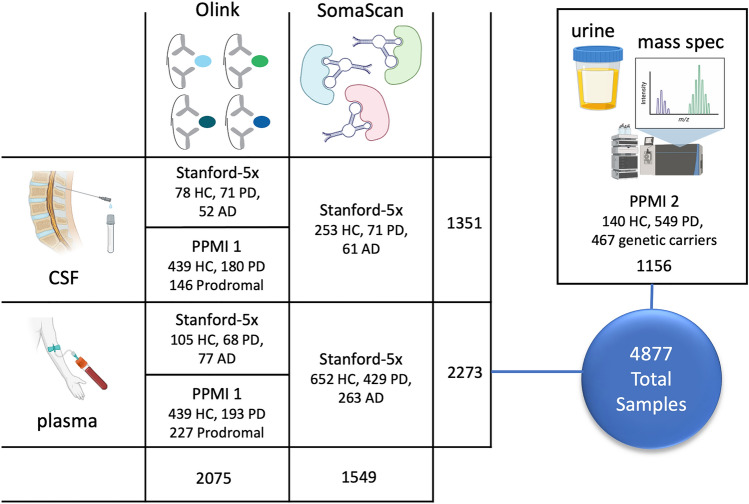
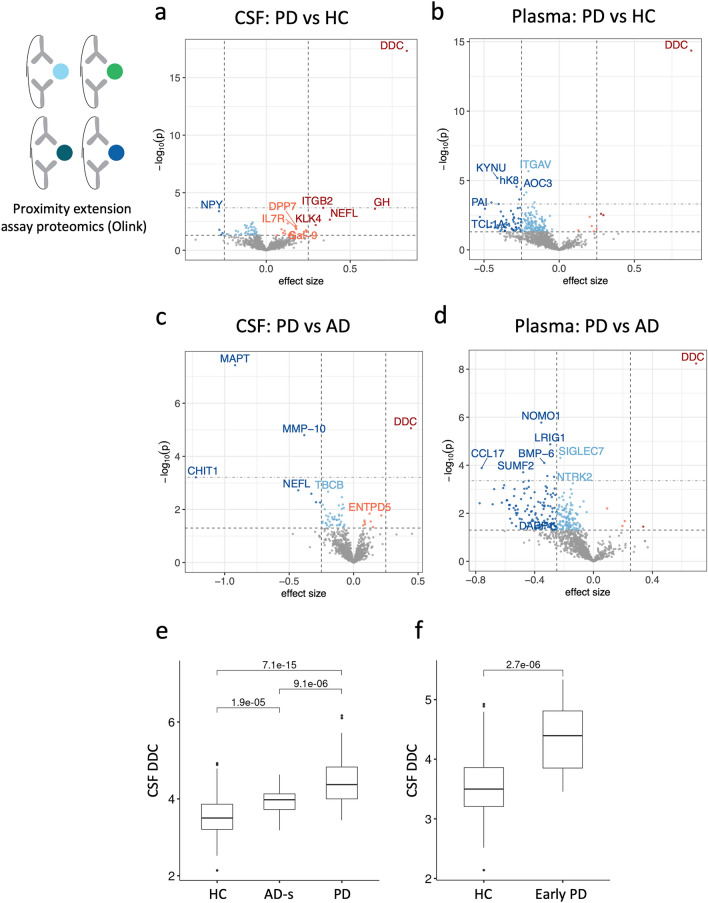
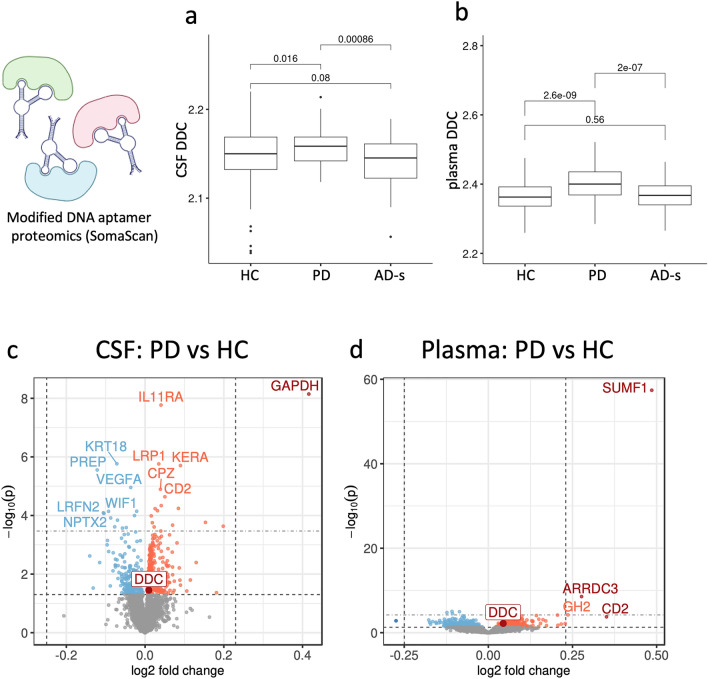
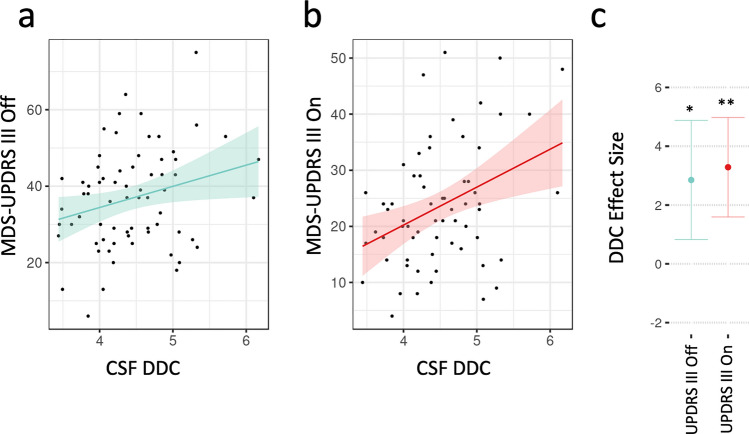
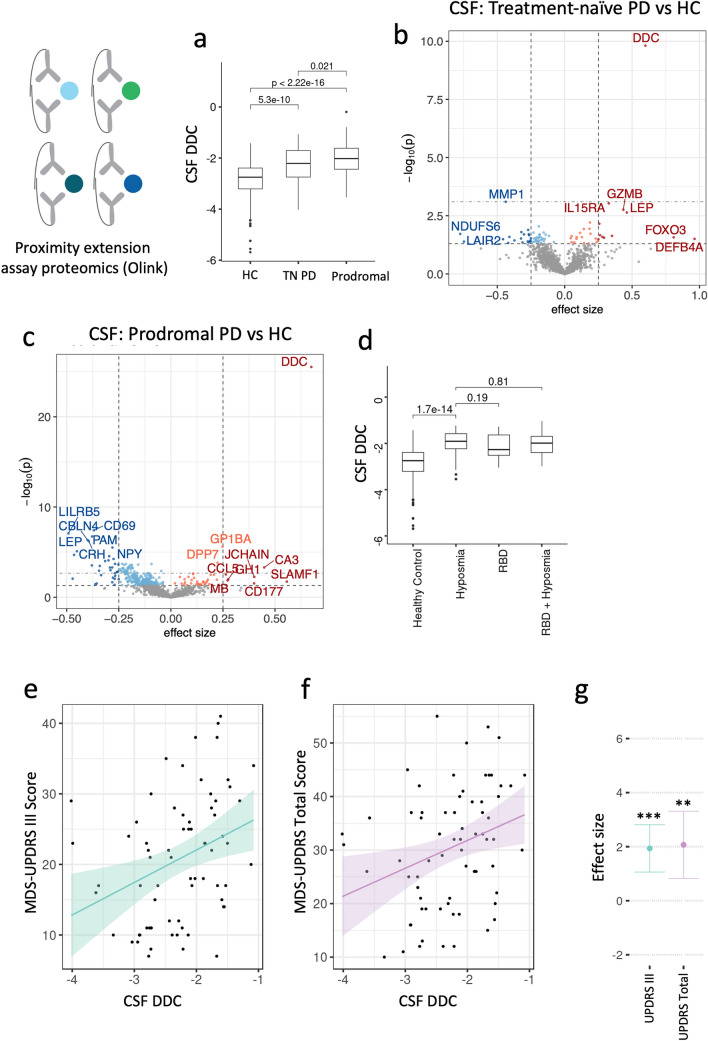
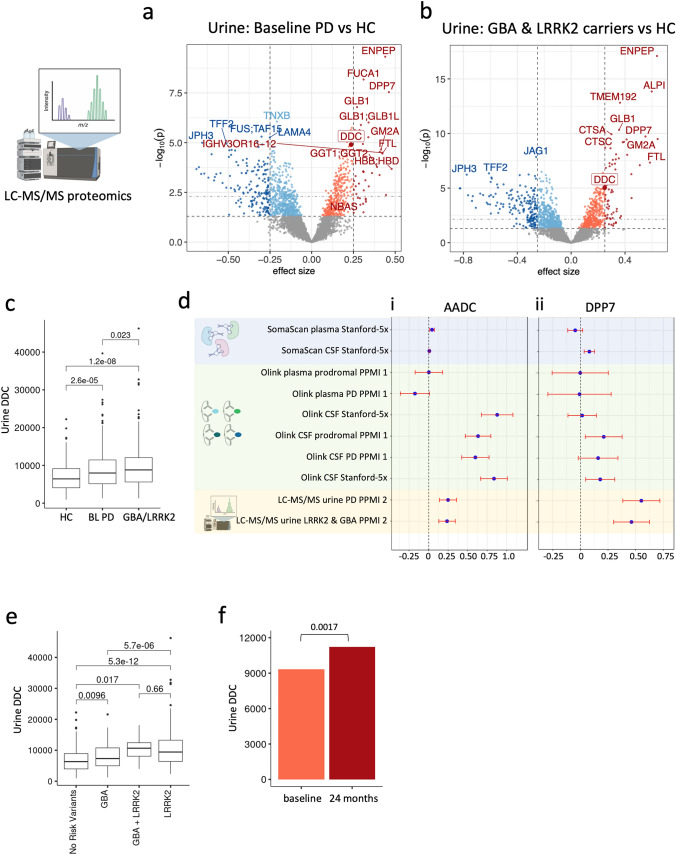
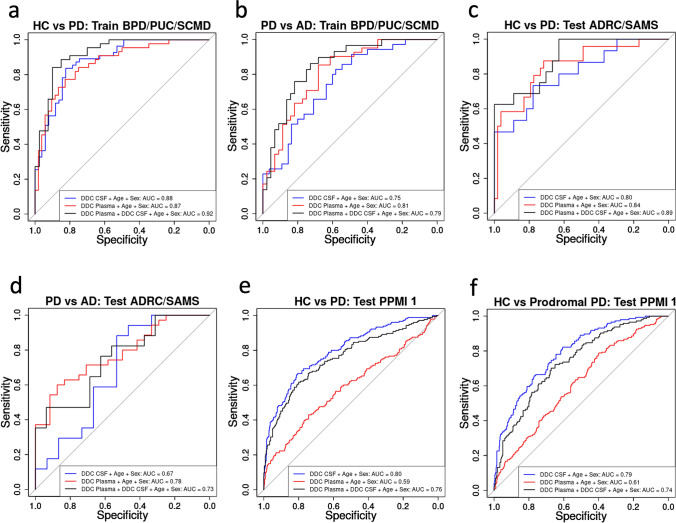
Parkinson's disease (PD) starts at the molecular and cellular level long before motor symptoms appear, yet there are no early-stage molecular biomarkers for diagnosis, prognosis prediction, or monitoring therapeutic response. This lack of biomarkers greatly impedes patient care and translational research-L-DOPA remains the standard of care more than 50 years after its introduction. Here, we performed a large-scale, multi-tissue, and multi-platform proteomics study to identify new biomarkers for early diagnosis and disease monitoring in PD. We analyzed 4877 cerebrospinal fluid, blood plasma, and urine samples from participants across seven cohorts using three orthogonal proteomics methods: Olink proximity extension assay, SomaScan aptamer precipitation assay, and liquid chromatography-mass spectrometry proteomics. We discovered that hundreds of proteins were upregulated in the CSF, blood, or urine of PD patients, prodromal PD patients with DAT deficit and REM sleep behavior disorder or anosmia, and non-manifesting genetic carriers of LRRK2 and GBA mutations. We nominate multiple novel hits across our analyses as promising markers of early PD, including DOPA decarboxylase (DDC), also known as L-aromatic acid decarboxylase (AADC), sulfatase-modifying factor 1 (SUMF1), dipeptidyl peptidase 2/7 (DPP7), glutamyl aminopeptidase (ENPEP), WAP four-disulfide core domain 2 (WFDC2), and others. DDC, which catalyzes the final step in dopamine synthesis, particularly stands out as a novel hit with a compelling mechanistic link to PD pathogenesis. DDC is consistently upregulated in the CSF and urine of treatment-naïve PD, prodromal PD, and GBA or LRRK2 carrier participants by all three proteomics methods. We show that CSF DDC levels correlate with clinical symptom severity in treatment-naïve PD patients and can be used to accurately diagnose PD and prodromal PD. This suggests that urine and CSF DDC could be a promising diagnostic and prognostic marker with utility in both clinical care and translational research.
© 2024. The Author(s).
Conflict of interest statement
J.R., T.W-C, B.L., and K.P. have filed a patent application related to this work. J.R. and T.W-C. are advisors of Teal Omics, where they have an equity stake. K.P. is on the Scientific Advisory Board for Curasen, where she receives consulting fees and stock options. K.P. is on the Scientific Advisory Board for Amprion, where she receives stock options.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
