

Atypical Fibroxanthoma Treated with a Topical Combination of Imiquimod, Tazarotene, and 5-Fluorouracil
- PMID: 38467988
- PMCID: PMC11052744
- DOI: 10.1007/s13555-024-01127-x
Atypical Fibroxanthoma Treated with a Topical Combination of Imiquimod, Tazarotene, and 5-Fluorouracil
Abstract
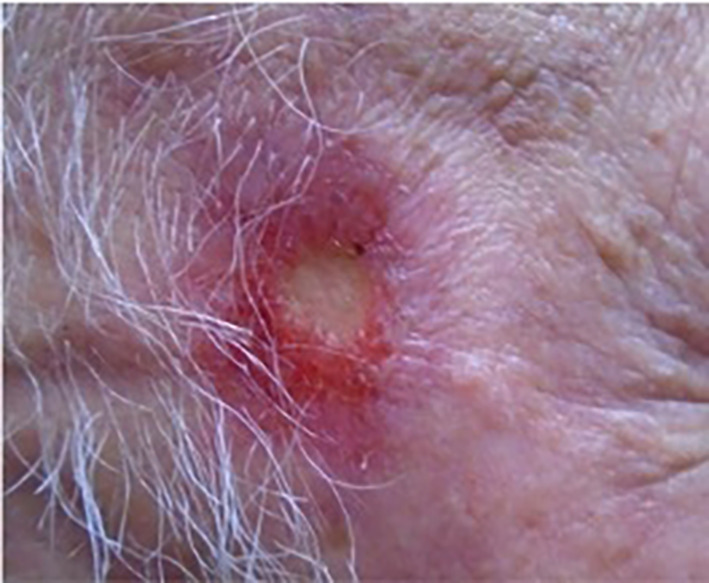
This case report describes an 80-year-old man who presented with a growing erythematous nodule with erosion, measuring 0.6 cm × 0.6 cm, on his right temple. This lesion was later diagnosed as atypical fibroxanthoma (AFX). Instead of undergoing Mohs surgery, the gold standard treatment, the patient opted to pursue a topical treatment regimen because of financial costs associated with surgical removal and repair. This topical regimen consisted of tazarotene cream, imiquimod cream, and 5-fluorouracil solution, applied for 30 days. The patient was directed to use this combination 5 days per week for 6 weeks. The specified dosage for each medication was a fifth of a packet of imiquimod 5% cream, an equivalent amount of tazarotene 0.1% cream, and a single drop of 5-fluorouracil 2% solution. These were combined on a bandage and placed on the lesion overnight. Following the treatment, a 3-week post-application examination revealed an erosion, 1.0 cm × 0.9 cm, amidst erythema. A subsequent incisional biopsy with histopathology and stains for CD10 and CD99, 3 weeks after treatment, and three punch biopsies with histopathology and stains for CD10 and CD99, 1-year post-treatment, confirmed the absence of AFX. AFX is a superficial variant of pleomorphic dermal sarcoma (PDS), which shares histologic similarities, yet the exact relationship between AFX/PDS and undifferentiated pleomorphic sarcoma is still not well understood. Previous studies have indicated a genomic similarity between AFX/PDS and cutaneous squamous cell carcinoma (cSCC), which suggests the potential efficacy of cSCC-targeted treatments for AFX/PDS. This case marks the first recorded instance of successful topical medical treatment of AFX, offering an alternative for patients who may opt out of surgical intervention. Continued research to assess the broader efficacy of this approach is encouraged.
Keywords: 5-fluorouracil; Atypical fibroxanthoma; Imiquimod; Nonsurgical; Tazarotene; Topical therapy.
© 2024. The Author(s).
Conflict of interest statement
William J. Nahm, Evangelos V. Badiavas, Robert S. Kirsner, Carter J. Boyd, Anita A. Arthur, Sean Bae, and John Shen have nothing to disclose.
Figures



Similar articles
-
Increase of atypical fibroxanthoma and pleomorphic dermal sarcoma: a retrospective analysis of four German skin cancer centers.J Dtsch Dermatol Ges. 2022 Dec;20(12):1581-1588. doi: 10.1111/ddg.14911. Epub 2022 Nov 28. J Dtsch Dermatol Ges. 2022. PMID: 36442137
-
Conception and Management of a Poorly Understood Spectrum of Dermatologic Neoplasms: Atypical Fibroxanthoma, Pleomorphic Dermal Sarcoma, and Undifferentiated Pleomorphic Sarcoma.Curr Treat Options Oncol. 2017 Aug;18(8):50. doi: 10.1007/s11864-017-0489-6. Curr Treat Options Oncol. 2017. PMID: 28762020 Review.
-
Atypical fibroxanthoma and pleomorphic dermal sarcoma - gene expression analysis compared with undifferentiated cutaneous squamous cell carcinoma.J Dtsch Dermatol Ges. 2023 May;21(5):482-491. doi: 10.1111/ddg.15006. Epub 2023 Apr 10. J Dtsch Dermatol Ges. 2023. PMID: 37035902
-
Pleomorphic Dermal Sarcoma: A Clinical and Histopathologic Emulator of Atypical Fibroxanthoma, but Different Biologic Behavior.HCA Healthc J Med. 2022 Oct 31;3(5):299-304. doi: 10.36518/2689-0216.1334. eCollection 2022. HCA Healthc J Med. 2022. PMID: 37425251 Free PMC article.
-
Pleomorphic dermal sarcoma in a man with HIV: report with next-generation sequencing analysis and review of the atypical fibroxanthoma/pleomorphic dermal sarcoma spectrum.Dermatol Online J. 2019 Nov 15;25(11):13030/qt8p66q9fv. Dermatol Online J. 2019. PMID: 32045146 Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
