

Nonketotic hyperglycemia hemichorea and hemiballismus: a case report
- PMID: 38468351
- PMCID: PMC10929169
- DOI: 10.1186/s13256-023-04332-y
Nonketotic hyperglycemia hemichorea and hemiballismus: a case report
Abstract
Background: Diabetic striatopathy, also known as hyperglycemic hemichorea-hemiballismus, is a rare movement disorder associated with nonketotic hyperglycemia in patients with poorly controlled diabetes mellitus. The pathophysiology is not fully elucidated but may involve hyperviscosity, ischemia, and alterations in basal ganglia neurotransmitters.
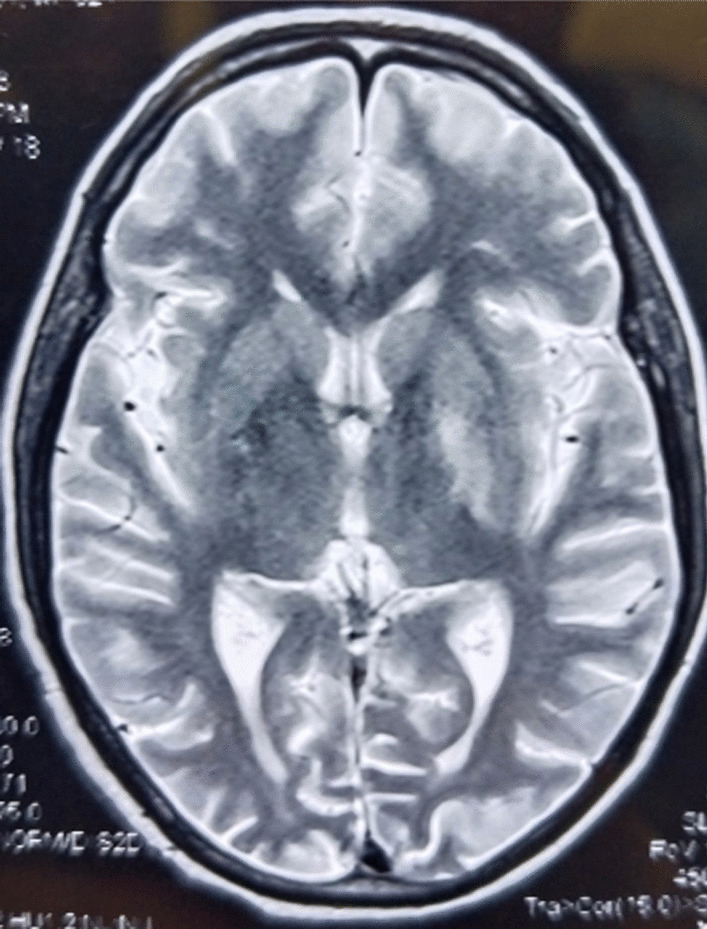
Case presentation: We present a case of a 64-year-old Asian female patient with longstanding poorly controlled type 2 diabetes mellitus who developed abrupt-onset right-sided hemichorea-hemiballismus. Laboratory results showed hyperglycemia without ketoacidosis. Neuroimaging revealed left putaminal hyperdensity on computed tomography and T1 hyperintensity on magnetic resonance imaging. With insulin therapy and tetrabenazine, her movements improved but persisted at 1-month follow-up.
Discussion: This case illustrates the typical features of diabetic striatopathy, including acute choreiform movements contralateral to neuroimaging abnormalities in the setting of nonketotic hyperglycemia. While neuroleptics may provide symptomatic relief, prompt glycemic control is critical given the risk of recurrence despite imaging normalization.
Conclusion: Diabetic striatopathy should be recognized as a rare disorder that can occur with poorly controlled diabetes. Further study of its pathophysiological mechanisms is needed to better guide management. Maintaining tight glycemic control is essential to prevent recurrence of this debilitating movement disorder.
Keywords: Acute choreiform movements; Diabetic striatopathy; Hyperglycemic hemichorea-hemiballismus; Neurotransmitter alterations; Nonketotic hyperglycemia; Putaminal hyperdensity; Type 2 diabetes mellitus.
© 2024. The Author(s).
Conflict of interest statement
No potential competing interests is relevant to this article.
Figures

Similar articles
-
Diabetic Striatopathy (Hyperglycemic Hemichorea-Hemiballismus Syndrome) in a Young Patient with Type 1 Diabetes Mellitus in Dar es Salaam, Tanzania: A Case Report.Case Rep Neurol. 2024 Nov 25;16(1):304-309. doi: 10.1159/000542452. eCollection 2024 Jan-Dec. Case Rep Neurol. 2024. PMID: 39981213 Free PMC article.
-
Diabetic striatopathy: a case report.Neurocase. 2023 Jun;29(3):90-91. doi: 10.1080/13554794.2024.2317788. Epub 2024 Feb 17. Neurocase. 2023. PMID: 38367007
-
Is diabetic striatopathy the culprit of seizures in a patient with ketotic hyperglycemia-induced hemichorea-hemiballismus?BMC Neurol. 2022 Apr 8;22(1):133. doi: 10.1186/s12883-022-02659-5. BMC Neurol. 2022. PMID: 35395738 Free PMC article.
-
Neuroimaging of Diabetic Striatopathy: More Questions than Answers.Eur Neurol. 2022;85(5):371-376. doi: 10.1159/000524936. Epub 2022 Jun 17. Eur Neurol. 2022. PMID: 35717942 Review.
-
Hyperglycemic hemichorea due to diabetic striatopathy: case-based review.Curr Med Res Opin. 2022 Mar;38(3):365-369. doi: 10.1080/03007995.2021.2015159. Epub 2021 Dec 14. Curr Med Res Opin. 2022. PMID: 34873977 Review.
Cited by
-
A Case of Non-ketotic Hyperglycemic Hemichorea-Hemiballismus in a 54-Year-Old Male Individual With Type 2 Diabetes Mellitus.Cureus. 2025 Jan 22;17(1):e77820. doi: 10.7759/cureus.77820. eCollection 2025 Jan. Cureus. 2025. PMID: 39991375 Free PMC article.
-
Diabetic Striatopathy: A Rare Case of Non-ketotic Hyperglycaemia-Induced Hemichorea.Cureus. 2025 Aug 4;17(8):e89384. doi: 10.7759/cureus.89384. eCollection 2025 Aug. Cureus. 2025. PMID: 40918801 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
