

Neonatal magnesium sulphate for neuroprotection: A systematic review and meta-analysis
- PMID: 38468452
- PMCID: PMC11579813
- DOI: 10.1111/dmcn.15899
Neonatal magnesium sulphate for neuroprotection: A systematic review and meta-analysis
Abstract
Aim: To review the evidence of the effects of neonatal magnesium sulphate for neuroprotection in perinatal asphyxia and hypoxic-ischaemic encephalopathy (HIE).
Method: This was a systematic review of randomized controlled trials (RCTs) (with meta-analysis) and non-RCTs assessing magnesium sulphate for treating perinatal asphyxia and HIE at 35 weeks or more gestation (primary outcomes: neonatal death and death or long-term major neurodevelopmental disability).
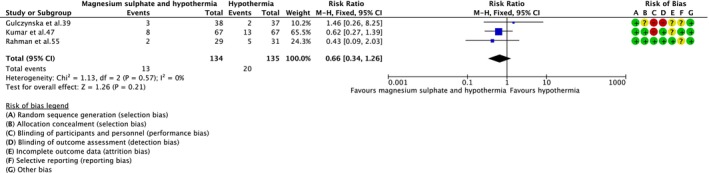
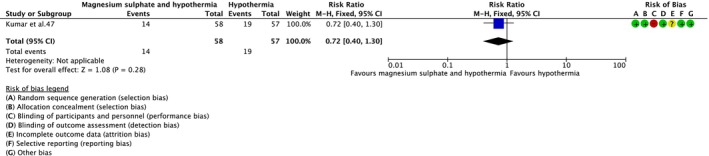
Results: Twenty-five RCTs (2099 infants) and four non-RCTs (871 infants) were included, 23 in low- and middle-income countries (LMICs). In RCTs, reductions in neonatal death with magnesium sulphate versus placebo or no treatment (risk ratio [RR] = 0.68; 95% confidence interval [CI] = 0.53-0.86; 13 RCTs), and magnesium sulphate with melatonin versus melatonin alone (RR = 0.74; 95% CI = 0.58-0.95; one RCT) were observed. No difference in neonatal death was seen for magnesium sulphate with therapeutic hypothermia versus therapeutic hypothermia alone (RR = 0.66, 95% CI = 0.34-1.26; three RCTs), or magnesium sulphate versus phenobarbital (RR = 3.00; 95% CI = 0.86-10.46; one RCT). No reduction in death or long-term neurodevelopmental disability (RR = 0.52; 95% CI = 0.14-1.89; one RCT) but reductions in several short-term adverse outcomes were observed with magnesium sulphate. Evidence was low- to very-low certainty because of risk of bias and imprecision.
Interpretation: Given the uncertainty of the current evidence, further robust neonatal magnesium sulphate research is justified. This may include high-quality studies to determine stand-alone effects in LMICs and effects with and after therapeutic hypothermia in high-income countries.
© 2024 The Authors. Developmental Medicine & Child Neurology published by John Wiley & Sons Ltd on behalf of Mac Keith Press.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article to disclose.
Figures


Similar articles
-
Antenatal and intrapartum interventions for preventing cerebral palsy: an overview of Cochrane systematic reviews.Cochrane Database Syst Rev. 2017 Aug 8;8(8):CD012077. doi: 10.1002/14651858.CD012077.pub2. Cochrane Database Syst Rev. 2017. PMID: 28786098 Free PMC article.
-
Different treatment regimens of magnesium sulphate for tocolysis in women in preterm labour.Cochrane Database Syst Rev. 2015 Dec 14;2015(12):CD011200. doi: 10.1002/14651858.CD011200.pub2. Cochrane Database Syst Rev. 2015. PMID: 26662716 Free PMC article.
-
Prophylactic barbiturate use for the prevention of morbidity and mortality following perinatal asphyxia.Cochrane Database Syst Rev. 2016 May 5;2016(5):CD001240. doi: 10.1002/14651858.CD001240.pub3. Cochrane Database Syst Rev. 2016. PMID: 27149645 Free PMC article.
-
Treatment for women with postpartum iron deficiency anaemia.Cochrane Database Syst Rev. 2024 Dec 13;12(12):CD010861. doi: 10.1002/14651858.CD010861.pub3. Cochrane Database Syst Rev. 2024. PMID: 39670550
-
Magnesium sulphate for women at term for neuroprotection of the fetus.Cochrane Database Syst Rev. 2013 Feb 28;2013(2):CD009395. doi: 10.1002/14651858.CD009395.pub2. Cochrane Database Syst Rev. 2013. PMID: 23450601 Free PMC article.
Cited by
-
Neuroprotection for neonatal hypoxic-ischemic encephalopathy: A review of novel therapies evaluated in clinical studies.Dev Med Child Neurol. 2025 May;67(5):591-599. doi: 10.1111/dmcn.16184. Epub 2024 Nov 20. Dev Med Child Neurol. 2025. PMID: 39563426 Free PMC article. Review.
-
Metabotropic glutamate receptors-guardians and gatekeepers in neonatal hypoxic-ischemic brain injury.Pharmacol Rep. 2024 Dec;76(6):1272-1285. doi: 10.1007/s43440-024-00653-x. Epub 2024 Sep 17. Pharmacol Rep. 2024. PMID: 39289333 Free PMC article. Review.
References
-
- World Health Organization (WHO) . Newborns: improving survival and well‐being. Available from: https://www.who.int/news‐room/fact‐sheets/detail/newborns‐reducing‐morta....
-
- McIntyre S, Nelson KB, Mulkey SB, Lechpammer M, Molloy E, Badawi N. Neonatal encephalopathy: focus on epidemiology and underexplored aspects of etiology. Semin Fetal Neonatal Med 2021; 26: 101265. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
