

Influence of Race/Ethnicity and Sex on Coronary Stent Outcomes in Diabetic Patients
- PMID: 38469035
- PMCID: PMC10927016
- DOI: 10.1016/j.jscai.2023.101053
Influence of Race/Ethnicity and Sex on Coronary Stent Outcomes in Diabetic Patients
Abstract
Background: How diabetes mellitus (DM), race/ethnicity, and sex impact ischemic events following coronary artery stent procedures is unknown.
Methods: Using the PLATINUM Diversity and PROMUS Element Plus Post-Approval Pooled Study (N = 4184), we examined the impact of race/ethnicity, sex, and DM on coronary stent outcomes. Primary outcome was 1-year major adverse cardiac events (MACE) (MACE composite: death, myocardial infarction [MI], and target vessel revascularization).
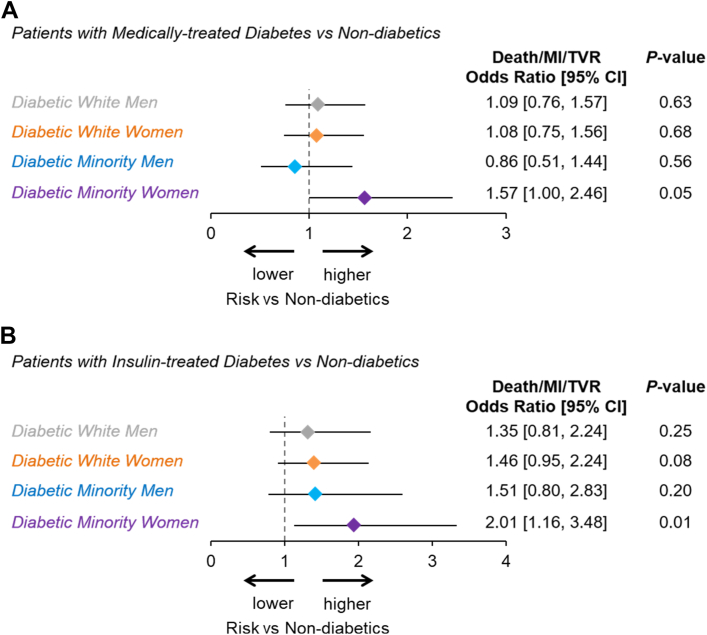
Results: The study sample included 1437 diabetic patients (501 White men, 470 White women, 246 minority men, 220 minority women) and 2641 patients without medically treated DM (561 minority, 1090 women). Mean age (years) ranged from 61 in minority men to 65 in White women. Diabetic patients had a higher prevalence of atherosclerotic risk factors and comorbidities. Diabetic minority women (DMW; 70% Black, 27% Hispanic) had similar atherosclerotic risk factors to other diabetics, but experienced higher 1-year MACE (14.4% vs 7.5%, P <.01) and MI (4.3% vs 1.6%, P <.01) rates compared with patients without medically treated DM. No other diabetic cohort (White men, White women, minority men) showed an increased risk of MACE vs patients without medically treated DM. The incremental risk of MACE in DMW was associated with insulin use and persisted after risk adjustment (adjusted odds ratio 1.6 vs patients without medically treated DM; 95% CI, 1.0-2.5). Independent predictors of 1-year MACE included insulin use, hyperlipidemia, renal disease, and prior MI.
Conclusions: DMW face the highest risk of ischemic events following coronary stenting, driven, in part, by insulin use. Aggressive secondary prevention and strict glycemic control are imperative in this cohort, and further research is warranted to elucidate the biologic mechanisms underpinning these observations.
Clinical trial registration: NCT02240810 (http://clinicaltrials.gov/).
Keywords: coronary; diabetes; minority; outcomes; stent; women.
Figures





Comment in
-
The Importance of Equity in Health Care.J Soc Cardiovasc Angiogr Interv. 2023 Aug 4;2(5):101065. doi: 10.1016/j.jscai.2023.101065. eCollection 2023 Sep-Oct. J Soc Cardiovasc Angiogr Interv. 2023. PMID: 39132409 Free PMC article. No abstract available.
References
-
- Moussa I., Leon M.B., Baim D.S., et al. Impact of sirolimus-eluting stents on outcome in diabetic patients: a SIRIUS (SIRolImUS-coated Bx Velocity balloon-expandable stent in the treatment of patients with de novo coronary artery lesions) substudy. Circulation. 2004;109(19):2273–2278. doi: 10.1161/01.CIR.0000129767.45513.71. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
