

Cystic Adenomyoma in Pregnancy: A Case Report
- PMID: 38469356
- PMCID: PMC10926917
- DOI: 10.2147/IJWH.S450701
Cystic Adenomyoma in Pregnancy: A Case Report
Abstract
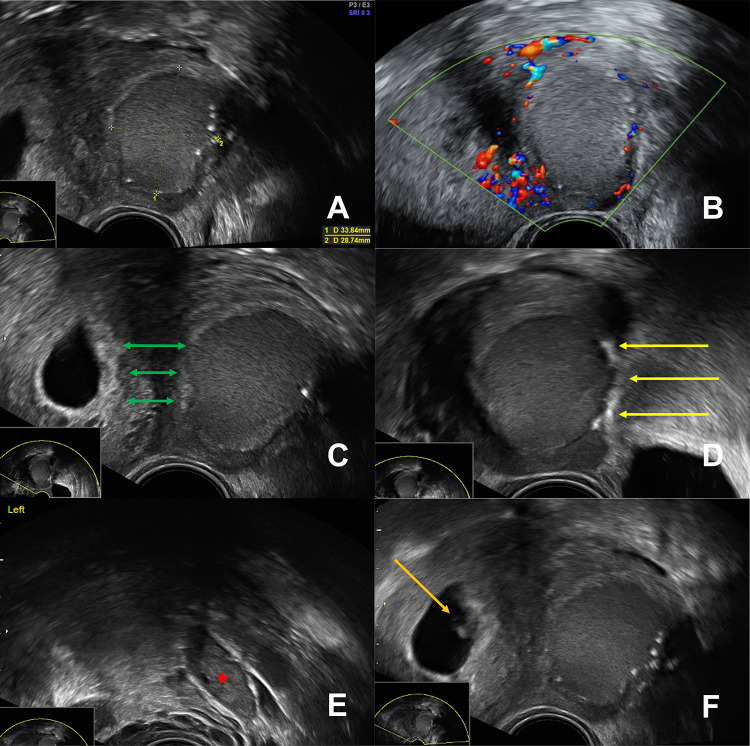
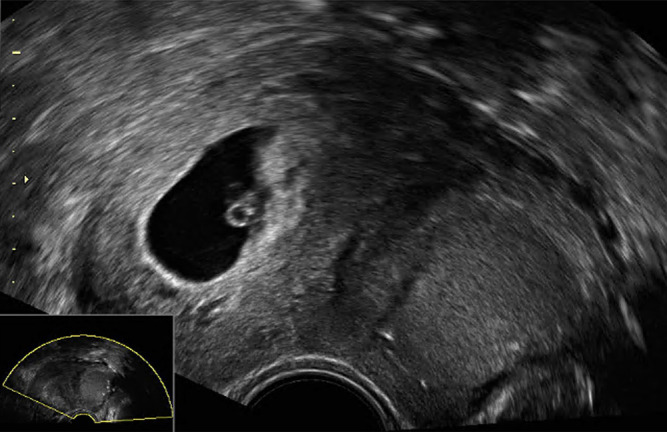
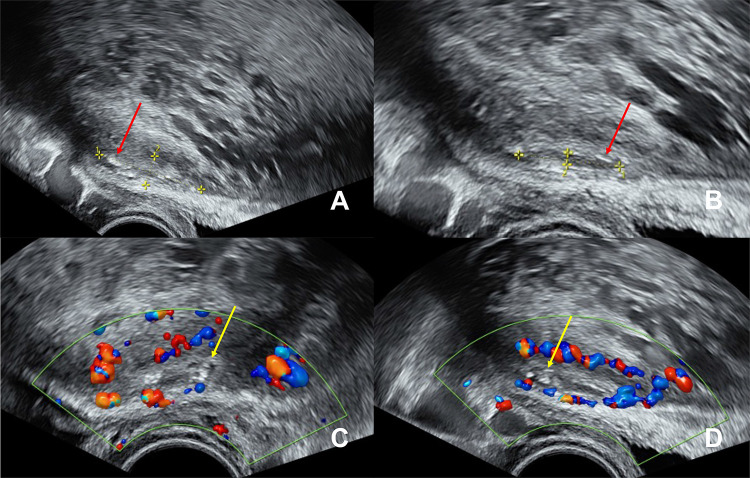
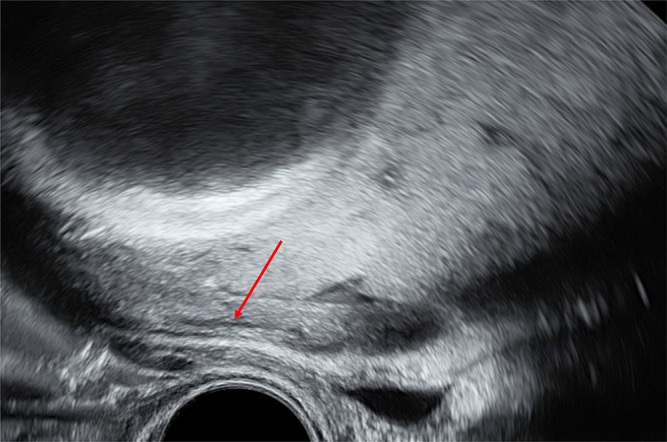
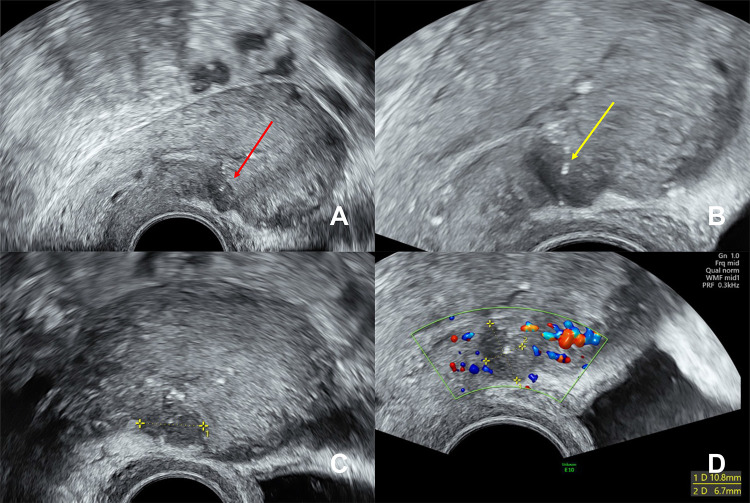
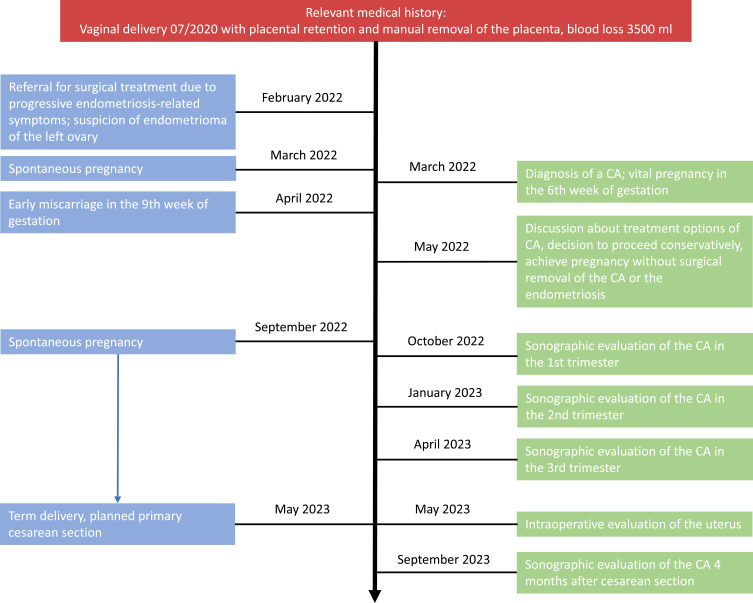
Cystic adenomyomas (CA) are rare. They primarily affect adolescents and young women in their fertile years. Therefore, fertility and pregnancy outcome are of pivotal relevance in this patient collective. Apart from the guidelines of the European Society of Human Reproduction and Embryology (ESHRE) on the management of endometriosis in general, there are no specific treatment recommendations for CA and, as far as our research shows, no data illustrating the behavior of a CA over the course of pregnancy. Thus, we report the case of a 32-year-old 1-gravida, 1-para, preconceptionally diagnosed with a CA by ultrasound. After thoroughly discussing further treatment options, the decision was made to opt for a more conservative approach and not perform surgery before attempting a next pregnancy. The patient conceived spontaneously and sonographic monitoring of the CA throughout pregnancy showed complete regression of the cystic component during the second trimester. A healthy baby was delivered at term by an uncomplicated elective cesarean section. Following a review of the literature and taking into account the course of our case, we propose the feasibility of a conservative, non-surgical approach in women with a CA and the desire to conceive.
Keywords: conservative management; cystic adenomyoma; endometriosis; fertility; pregnancy.
© 2024 Verta et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures

Similar articles
-
Fertility after conservative surgery for adenomyomas.Hum Reprod. 1993 Oct;8(10):1708-10. doi: 10.1093/oxfordjournals.humrep.a137919. Hum Reprod. 1993. PMID: 8300834
-
Cystic adenomyoma surgery.J Gynecol Obstet Hum Reprod. 2022 Mar;51(3):102313. doi: 10.1016/j.jogoh.2022.102313. Epub 2022 Jan 11. J Gynecol Obstet Hum Reprod. 2022. PMID: 35031510
-
Successful pregnancy following conservative management of low-grade endometrial stromal sarcoma: A case report.Oncol Lett. 2014 Apr;7(4):1039-1042. doi: 10.3892/ol.2014.1858. Epub 2014 Feb 7. Oncol Lett. 2014. PMID: 24944665 Free PMC article.
-
Surgical techniques for excision of juvenile cystic adenomyoma.Fertil Steril. 2022 Oct;118(4):810-811. doi: 10.1016/j.fertnstert.2022.06.025. Epub 2022 Aug 3. Fertil Steril. 2022. PMID: 35931491 Review.
-
Reproductive outcomes following cesarean scar pregnancy - a case series and review of the literature.Eur J Obstet Gynecol Reprod Biol. 2016 May;200:102-7. doi: 10.1016/j.ejogrb.2016.02.039. Epub 2016 Mar 8. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 27014853 Review.
Cited by
-
A Rare Case of Multiple Subserous Uterine Adenomyomas Misdiagnosed as an Ovarian Cyst, Diagnosed and Treated by Laparoscopy.Int J Womens Health. 2024 Dec 19;16:2203-2208. doi: 10.2147/IJWH.S494745. eCollection 2024. Int J Womens Health. 2024. PMID: 39720675 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
