

Pseudomonas aeruginosa ventricular assist device infections: findings from ineffective phage therapies in five cases
- PMID: 38470133
- PMCID: PMC10989018
- DOI: 10.1128/aac.01728-23
Pseudomonas aeruginosa ventricular assist device infections: findings from ineffective phage therapies in five cases
Erratum in
-
Erratum for Aslam et al., "Pseudomonas aeruginosa ventricular assist device infections: findings from ineffective phage therapies in five cases".Antimicrob Agents Chemother. 2025 Feb 13;69(2):e0180024. doi: 10.1128/aac.01800-24. Epub 2025 Jan 8. Antimicrob Agents Chemother. 2025. PMID: 39772863 Free PMC article. No abstract available.
Abstract
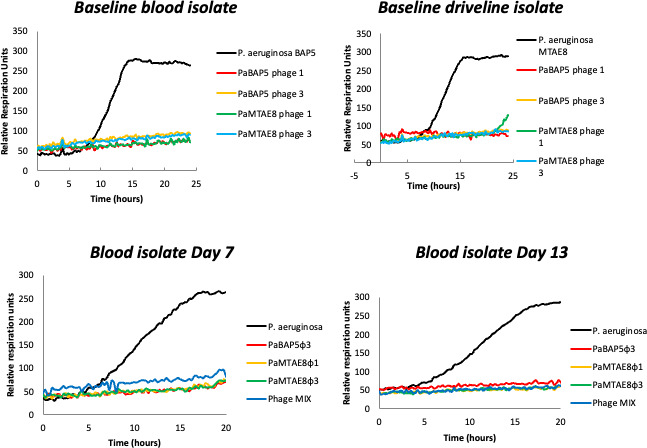
Left ventricular assist devices (LVAD) are increasingly used for management of heart failure; infection remains a frequent complication. Phage therapy has been successful in a variety of antibiotic refractory infections and is of interest in treating LVAD infections. We performed a retrospective review of four patients that underwent five separate courses of intravenous (IV) phage therapy with concomitant antibiotic for treatment of endovascular Pseudomonas aeruginosa LVAD infection. We assessed phage susceptibility, bacterial strain sequencing, serum neutralization, biofilm activity, and shelf-life of phage preparations. Five treatments of one to four wild-type virulent phage(s) were administered for 14-51 days after informed consent and regulatory approval. There was no successful outcome. Breakthrough bacteremia occurred in four of five treatments. Two patients died from the underlying infection. We noted a variable decline in phage susceptibility following three of five treatments, four of four tested developed serum neutralization, and prophage presence was confirmed in isolates of two tested patients. Two phage preparations showed an initial titer drop. Phage biofilm activity was confirmed in two. Phage susceptibility alone was not predictive of clinical efficacy in P. aeruginosa endovascular LVAD infection. IV phage was associated with serum neutralization in most cases though lack of clinical effect may be multifactorial including presence of multiple bacterial isolates with varying phage susceptibility, presence of prophages, decline in phage titers, and possible lack of biofilm activity. Breakthrough bacteremia occurred frequently (while the organism remained susceptible to administered phage) and is an important safety consideration.
Keywords: LVAD; MDRO; Pseudomonas aeruginosa; device-related infection; phage therapy.
Conflict of interest statement
Saima Aslam: Research funding support from the Cystic Fibrosis Foundation, Armata Pharmaceuticals, Adaptive Phage Therapeutics, and Contrafect Inc. Consultant for BiomX and Phico Therapeutics. Medical advisory board for Pherecydes Pharma and Phiogen. Dwayne Roach: none. Mikeljon P. Nikolich: Royalty-bearing Biological Material License Agreement with Adaptive Phage Therapeutics exists now but work presented in this manuscript predated it. Patent PCT/US22/73852, METHOD OF TREATING DRUG RESISTANT ESKAPE PATHOGENS USING THERAPEUTIC BACTERIOPHAGES was filed, but work reported in this manuscript predated the filing. Biswajit Biswas: Navy Work Unit # A1417. Dr. Biswas has a patent "Bacteriophage compositions and methods of selection of components against specific bacteria" US patent #10357522, which was licensed before. Robert T Schooley: Consulting fees from GSK, LyseNtech. Kimberley A. Lilly-Bishop: none. Gregory K. Rice: none. Regina Z. Cer: none. Theron Hamilton: none. Mathew Henry: Mr. Henry has a patent 10357522 licensed. Tiffany Luong: none. Ann-Charlott Salabarria: none. Laura Sisk-Hackworth: none. Andrey A. Filippov: Pending Patent PCT/US22/73852, METHOD OF TREATING DRUG RESISTANT ESKAPE PATHOGENS USING THERAPEUTIC BACTERIOPHAGES Francois Lebreton: none. Lindsey Hall: none. Ran Nir-Paz: Consultant for BiomX; and has participated and served as a PI and on Data Safety Monitoring Board for a clinical trial by Technophage. Hadil Onalla: none. Gilat Livni: none. Eran Shostak: none. Anat Weider-Feinsod: none. Dafna Yahav: none. Ortal Yerushalmy: none. Sivan Alkalay-Oren: none. Leron Khalifa: none. Amit Rimon: none. Daniel Gelman: none. Ronen Hazan: none.
Figures




References
-
- Molina EJ, Shah P, Kiernan MS, Cornwell WK, Copeland H, Takeda K, Fernandez FG, Badhwar V, Habib RH, Jacobs JP, Koehl D, Kirklin JK, Pagani FD, Cowger JA. 2021. The society of thoracic surgeons intermacs 2020 annual report. Ann Thorac Surg 111:778–792. doi: 10.1016/j.athoracsur.2020.12.038 - DOI - PubMed
-
- Tran H, Aslam S. 2021. Ventricular assist devices, ECMO, and cardiac support devices: challenges in the bridge to transplant. In Morris MI, Kotton CN, Wolfe CR (ed), Emerging transplant infections: clinical challenges and implications. Springer International Publishing, Cham.
-
- Suh GA, Lodise TP, Tamma PD, Knisely JM, Alexander J, Aslam S, Barton KD, Bizzell E, Totten KMC, Campbell JL, Chan BK, Cunningham SA, Goodman KE, Greenwood-Quaintance KE, Harris AD, Hesse S, Maresso A, Nussenblatt V, Pride D, Rybak MJ, Sund Z, van Duin D, Van Tyne D, Patel R, Antibacterial Resistance Leadership Group . 2022. Considerations for the use of phage therapy in clinical practice. Antimicrob Agents Chemother 66:e0207121. doi: 10.1128/AAC.02071-21 - DOI - PMC - PubMed
-
- Aslam S, Lampley E, Wooten D, Karris M, Benson C, Strathdee S, Schooley RT. 2020. Lessons learned from the first 10 consecutive cases of intravenous bacteriophage therapy to treat multidrug-resistant bacterial infections at a single center in the United States. Open Forum Infect Dis 7:ofaa389. doi: 10.1093/ofid/ofaa389 - DOI - PMC - PubMed
