

Prevalence and trajectories of neuropsychological post-COVID-19 symptoms in initially hospitalized patients
- PMID: 38470168
- PMCID: PMC10949081
- DOI: 10.2340/jrm.v56.25315
Prevalence and trajectories of neuropsychological post-COVID-19 symptoms in initially hospitalized patients
Abstract
Objective: To investigate the prevalence and trajectories of post-COVID-19 neuropsychological symptoms.
Design: Prospective longitudinal multicentre cohort study.
Subjects: A total of 205 patients initially hospitalized with SARS-CoV-2 (COVID-19).
Methods: Validated questionnaires were administered at 9 months (T1) and 15 months (T2) post-hospital discharge to assess fatigue, cognitive complaints, insomnia, anxiety, depression, and post-traumatic stress symptoms.
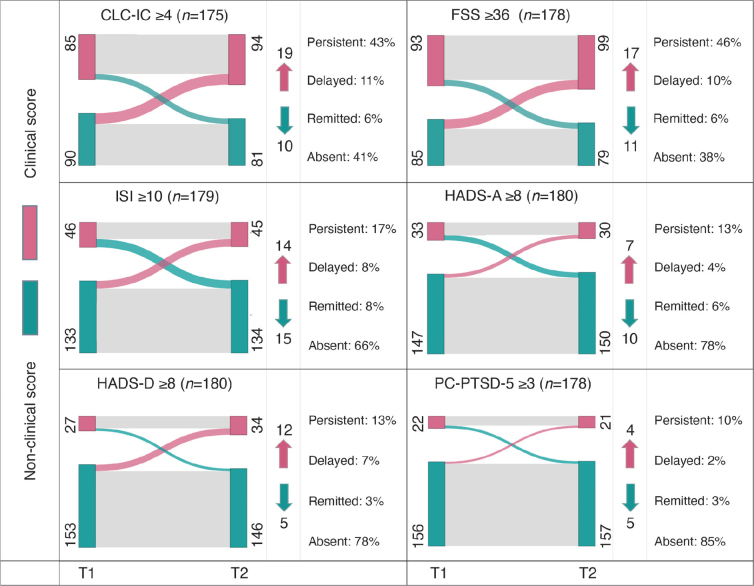
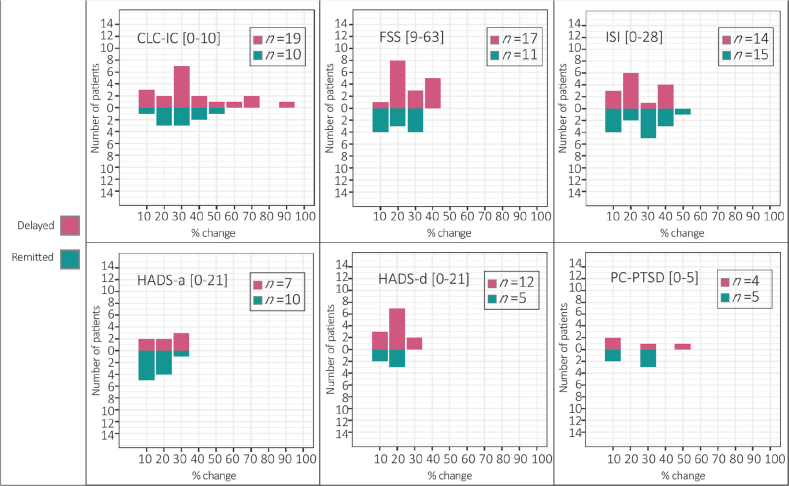
Results: Analyses included 184 out of 205 patients. Approximately 50% experienced high cognitive complaints at T1 and T2, while severe fatigue affected 52.5% at T1 and 55.6% at T2. Clinically relevant insomnia scores were observed in 25% of patients at both time-points. Clinically relevant anxiety scores were present in 18.3% at T1 and 16.7% at T2, depression in 15.0% at T1 and 18.9% at T2, and PTSD in 12.4% at T1 and 11.8% at T2. Most symptoms remained stable, with 59.2% of patients experiencing at least 1 persistent symptom. In addition, 31.5% of patients developed delayed-onset symptoms.
Conclusion: Post-COVID-19 cognitive complaints and fatigue are highly prevalent and often persist. A subgroup develops delayed symptoms. Emotional distress is limited. Screening can help identify most patients experiencing long-term problems. Future research should determine risk factors for persistent and delayed onset symptoms.
Conflict of interest statement
Figures
References
-
- Fernández-de-Las-Peñas C, Palacios-Ceña D, Gómez-Mayordomo V, Florencio LL, Cuadrado ML, Plaza-Manzano G, et al. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: a systematic review and meta-analysis. Eur J Intern Med 2021; 92: 55–70. DOI: 10.1016/j.ejim.2021.06.009 - DOI - PMC - PubMed
-
- Barker-Collo S, Jones K, Theadom A, Starkey N, Dowell A, McPherson K, et al. Neuropsychological outcome and its correlates in the first year after adult mild traumatic brain injury: a population-based New Zealand study. Brain Inj 2015; 29: 1604–1616. DOI: 10.3109/02699052.2015.1075143 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
