

Posoleucel in Kidney Transplant Recipients with BK Viremia: Multicenter, Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial
- PMID: 38470444
- PMCID: PMC11149047
- DOI: 10.1681/ASN.0000000000000329
Posoleucel in Kidney Transplant Recipients with BK Viremia: Multicenter, Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial
Abstract
Key Points:
Posoleucel was generally safe, well tolerated, and associated with a greater reduction of BK viremia compared with placebo.
BK viremia reduction occurred coincident with an increase in the circulating frequency of BK virus–specific T cells in posoleucel recipients.
The presence and persistence of posoleucel was confirmed by T-cell receptor variable β sequencing.
Background: Kidney transplant recipients with BK virus infection are at risk of developing BK virus–associated nephropathy, allograft rejection, and subsequent graft loss. There are no approved treatments for BK virus infection. Posoleucel is an off-the-shelf, allogeneic, multivirus-specific T-cell investigational therapy targeting BK virus, as well as five other opportunistic viruses: adenovirus, cytomegalovirus, Epstein–Barr virus, human herpesvirus 6, and John Cunningham virus.
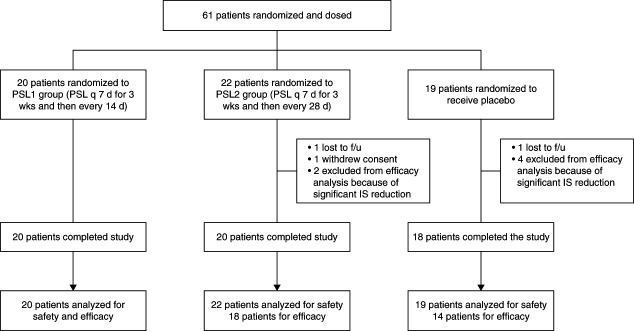
Methods: In this phase 2, double-blind study, kidney transplant recipients with BK viremia were randomized 1:1:1 to receive posoleucel weekly for 3 weeks and then every 14 days (bi-weekly dosing) or every 28 days (monthly dosing) or placebo for 12 weeks. Participants were followed for 12 weeks after completing treatment. The primary objective was safety; the secondary objective was plasma BK viral load reduction.
Results: Sixty-one participants were randomized and dosed. Baseline characteristics were similar across groups. No deaths, graft-versus-host disease, or cytokine release syndrome occurred. The proportion of patients who had adverse events (AEs) judged by the investigators to be treatment-related was slightly lower in recipients of posoleucel: 20% (4 of 20 patients) and 18% (4 of 22) in those infused on a bi-weekly and monthly schedule, respectively, and 26% (5 of 19) in placebo recipients. None of the grade 3–4 AEs or serious AEs in any group were deemed treatment-related. No deaths, graft-versus-host disease, or cytokine release syndrome occurred. Three participants had allograft rejection, but none were deemed treatment-related by investigators. In posoleucel recipients, BK viremia reduction was associated with an increase in the circulating frequency of BK virus–specific T cells, and the presence and persistence of posoleucel was confirmed by T-cell receptor sequencing.
Conclusions: Posoleucel was generally safe, well tolerated, and associated with a larger reduction of BK viremia compared with placebo. Limitations of this study include the relatively short duration of follow-up and lack of power to detect significant differences in clinical outcomes.
Clinical Trial registry name and registration number::
Study of Posoleucel (Formerly Known as ALVR105; Viralym-M) in Kidney Transplant Patients With BK Viremia,
Conflict of interest statement
D. Adey reports research funding from AlloVir, Hansa Pharmaceuticals, and Natera and honoraria from American Board of Internal Medicine. D. Adey reports advisory or leadership roles for American Society of Transplantation, OPTN/UNOS Policy Committee, Conflict of Interest Committee; Awards Committee; American Board of Internal Medicine, Subspecialty Governance Board; and
Figures



References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
