

Neutralizing IFN-γ autoantibodies are rare and pathogenic in HLA-DRB1*15:02 or 16:02 individuals
- PMID: 38470480
- PMCID: PMC11014650
- DOI: 10.1172/JCI178263
Neutralizing IFN-γ autoantibodies are rare and pathogenic in HLA-DRB1*15:02 or 16:02 individuals
Abstract
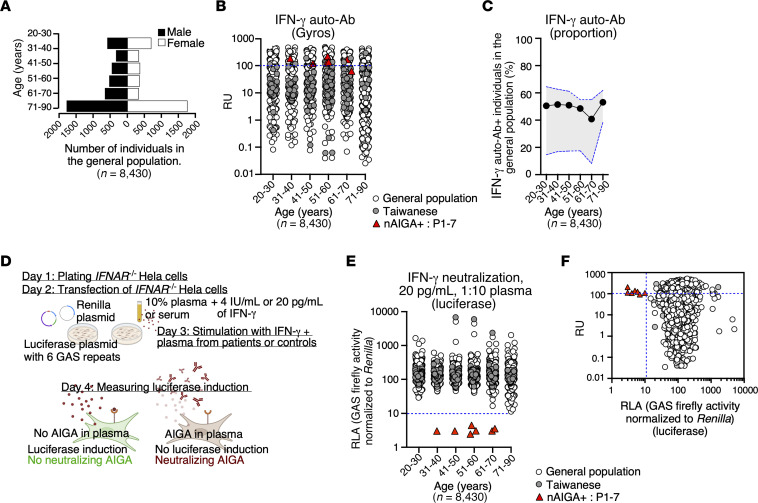
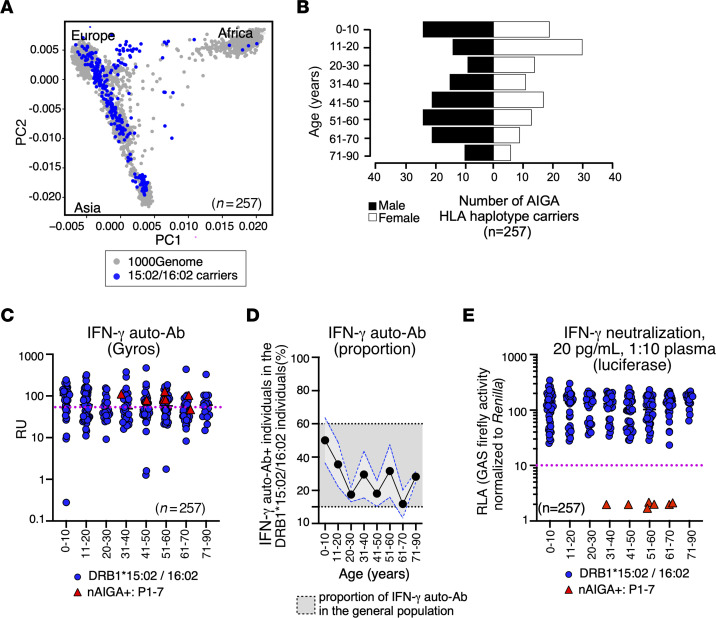
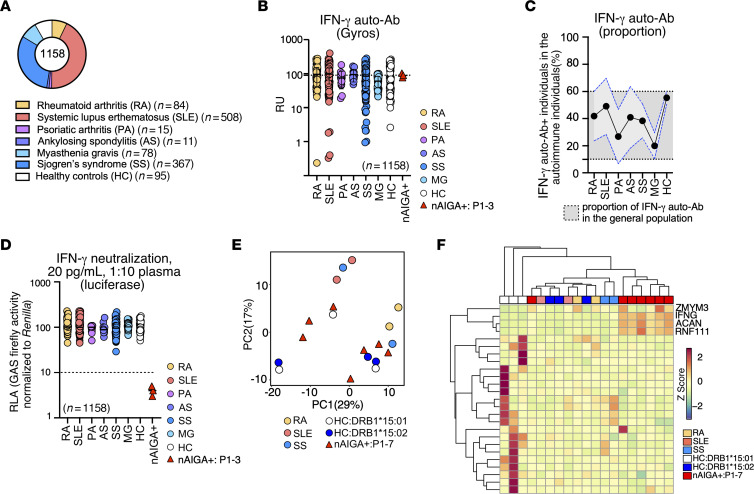
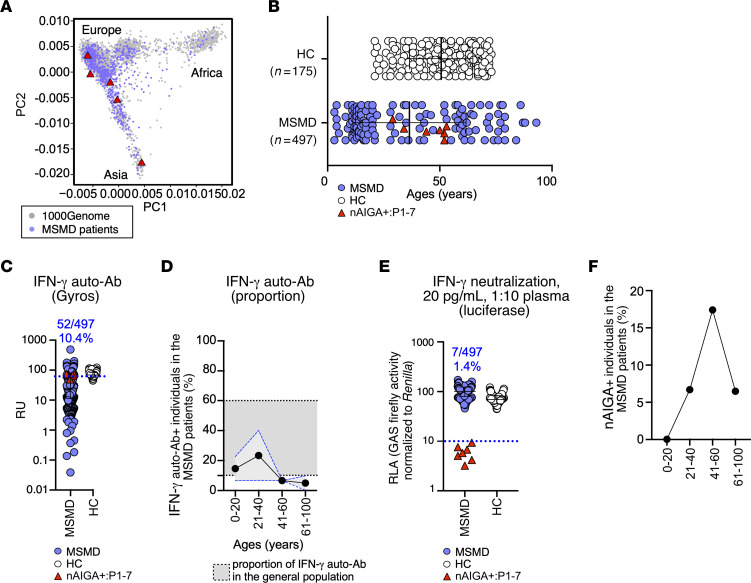
BACKGROUNDWeakly virulent environmental mycobacteria (EM) can cause severe disease in HLA-DRB1*15:02 or 16:02 adults harboring neutralizing anti-IFN-γ autoantibodies (nAIGAs). The overall prevalence of nAIGAs in the general population is unknown, as are the penetrance of nAIGAs in HLA-DRB1*15:02 or 16:02 individuals and the proportion of patients with unexplained, adult-onset EM infections carrying nAIGAs.METHODSThis study analyzed the detection and neutralization of anti-IFN-γ autoantibodies (auto-Abs) from 8,430 healthy individuals of the general population, 257 HLA-DRB1*15:02 or 16:02 carriers, 1,063 patients with autoimmune disease, and 497 patients with unexplained severe disease due to EM.RESULTSWe found that anti-IFN-γ auto-Abs detected in 4,148 of 8,430 healthy individuals (49.2%) from the general population of an unknown HLA-DRB1 genotype were not neutralizing. Moreover, we did not find nAIGAs in 257 individuals carrying HLA-DRB1* 15:02 or 16:02. Additionally, nAIGAs were absent in 1,063 patients with an autoimmune disease. Finally, 7 of 497 patients (1.4%) with unexplained severe disease due to EM harbored nAIGAs.CONCLUSIONThese findings suggest that nAIGAs are isolated and that their penetrance in HLA-DRB1*15:02 or 16:02 individuals is low, implying that they may be triggered by rare germline or somatic variants. In contrast, the risk of mycobacterial disease in patients with nAIGAs is high, confirming that these nAIGAs are the cause of EM disease.FUNDINGThe Laboratory of Human Genetics of Infectious Diseases is supported by the Howard Hughes Medical Institute, the Rockefeller University, the St. Giles Foundation, the National Institutes of Health (NIH) (R01AI095983 and U19AIN1625568), the National Center for Advancing Translational Sciences (NCATS), the NIH Clinical and Translational Science Award (CTSA) program (UL1 TR001866), the French National Research Agency (ANR) under the "Investments for the Future" program (ANR-10-IAHU-01), the Integrative Biology of Emerging Infectious Diseases Laboratory of Excellence (ANR-10-LABX-62-IBEID), ANR-GENMSMD (ANR-16-CE17-0005-01), ANR-MAFMACRO (ANR-22-CE92-0008), ANRSECTZ170784, the French Foundation for Medical Research (FRM) (EQU201903007798), the ANRS-COV05, ANR GENVIR (ANR-20-CE93-003), and ANR AI2D (ANR-22-CE15-0046) projects, the ANR-RHU program (ANR-21-RHUS-08-COVIFERON), the European Union's Horizon 2020 research and innovation program under grant agreement no. 824110 (EASI-genomics), the Square Foundation, Grandir - Fonds de solidarité pour l'enfance, the Fondation du Souffle, the SCOR Corporate Foundation for Science, the Battersea & Bowery Advisory Group, William E. Ford, General Atlantic's Chairman and Chief Executive Officer, Gabriel Caillaux, General Atlantic's Co-President, Managing Director, and Head of business in EMEA, and the General Atlantic Foundation, Institut National de la Santé et de la Recherche Médicale (INSERM) and of Paris Cité University. JR was supported by the INSERM PhD program for doctors of pharmacy (poste d'accueil INSERM). JR and TLV were supported by the Bettencourt-Schueller Foundation and the MD-PhD program of the Imagine Institute. MO was supported by the David Rockefeller Graduate Program, the Funai Foundation for Information Technology (FFIT), the Honjo International Scholarship Foundation (HISF), and the New York Hideyo Noguchi Memorial Society (HNMS).
Keywords: Autoimmune diseases; Cytokines; Genetics; Immunology.
Figures
Similar articles
-
Anti-IFN-γ autoantibodies in adults with disseminated nontuberculous mycobacterial infections are associated with HLA-DRB1*16:02 and HLA-DQB1*05:02 and the reactivation of latent varicella-zoster virus infection.Blood. 2013 Feb 21;121(8):1357-66. doi: 10.1182/blood-2012-08-452482. Epub 2012 Dec 13. Blood. 2013. PMID: 23243276
-
Clinical manifestations, course, and outcome of patients with neutralizing anti-interferon-γ autoantibodies and disseminated nontuberculous mycobacterial infections.Medicine (Baltimore). 2016 Jun;95(25):e3927. doi: 10.1097/MD.0000000000003927. Medicine (Baltimore). 2016. PMID: 27336882 Free PMC article.
-
HLA-DRB1 and HLA-DQB1 Are Associated with Adult-Onset Immunodeficiency with Acquired Anti-Interferon-Gamma Autoantibodies.PLoS One. 2015 May 26;10(5):e0128481. doi: 10.1371/journal.pone.0128481. eCollection 2015. PLoS One. 2015. PMID: 26011559 Free PMC article.
-
Autoimmune hepatitis, HLA and extended haplotypes.Autoimmun Rev. 2011 Feb;10(4):189-93. doi: 10.1016/j.autrev.2010.09.024. Epub 2010 Oct 7. Autoimmun Rev. 2011. PMID: 20933106 Review.
-
Cannabis: Effects of consumption on health [Internet].Paris (FR): Institut national de la santé et de la recherche médicale; 2001. Paris (FR): Institut national de la santé et de la recherche médicale; 2001. PMID: 21348165 Free Books & Documents. Review.
Cited by
-
A sensitive assay for measuring whole-blood responses to type I IFNs.Proc Natl Acad Sci U S A. 2024 Oct;121(40):e2402983121. doi: 10.1073/pnas.2402983121. Epub 2024 Sep 23. Proc Natl Acad Sci U S A. 2024. PMID: 39312669 Free PMC article.
-
Human immunity to fungal infections.J Exp Med. 2025 Jun 2;222(6):e20241215. doi: 10.1084/jem.20241215. Epub 2025 Apr 15. J Exp Med. 2025. PMID: 40232283 Review.
-
The monogenic landscape of human infectious diseases.J Allergy Clin Immunol. 2025 Mar;155(3):768-783. doi: 10.1016/j.jaci.2024.12.1078. Epub 2024 Dec 24. J Allergy Clin Immunol. 2025. PMID: 39724971 Review.
-
Serum IgE in the clinical features and disease outcomes of anti-interferon-γ autoantibodies syndrome.BMC Immunol. 2025 Mar 8;26(1):17. doi: 10.1186/s12865-025-00696-6. BMC Immunol. 2025. PMID: 40057680 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
