

Identification of four biotypes in temporal lobe epilepsy via machine learning on brain images
- PMID: 38472252
- PMCID: PMC10933450
- DOI: 10.1038/s41467-024-46629-6
Identification of four biotypes in temporal lobe epilepsy via machine learning on brain images
Abstract
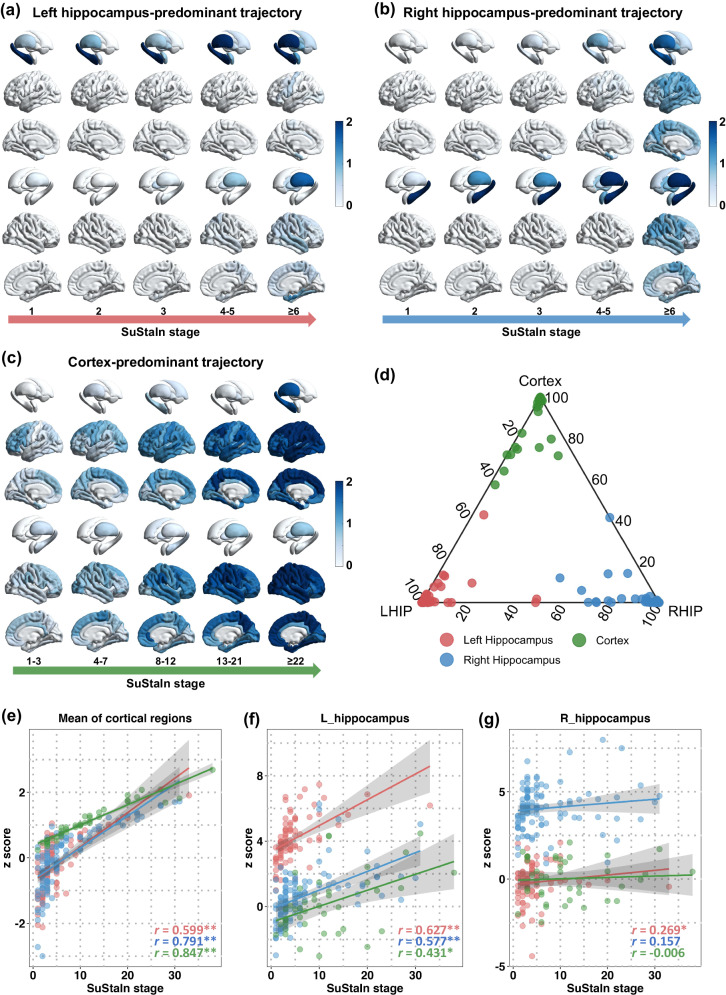
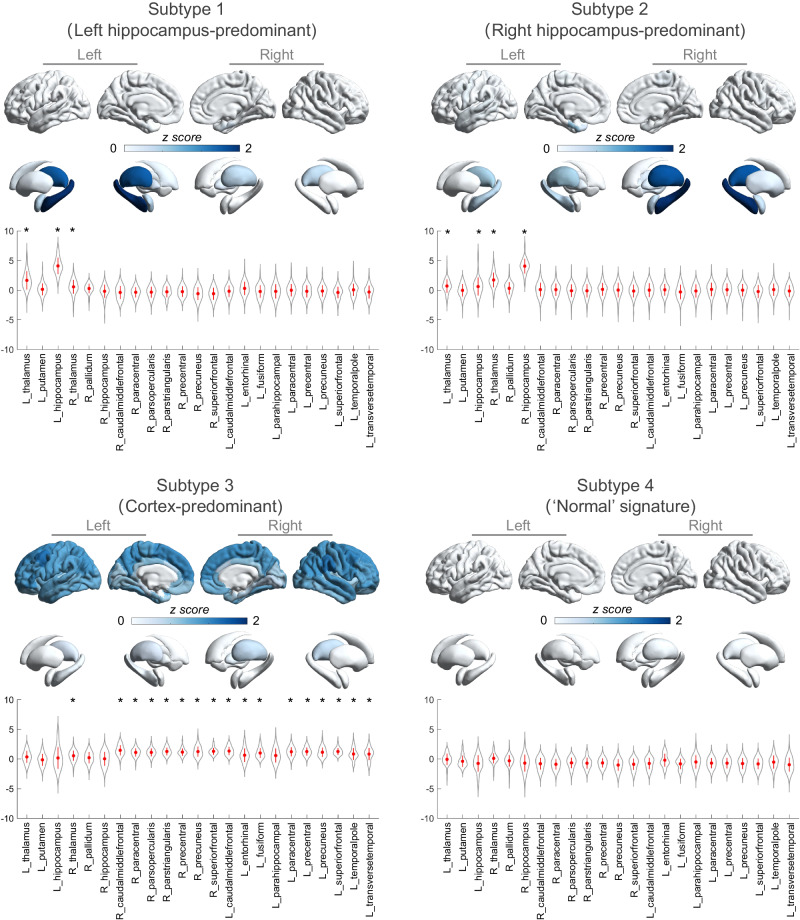
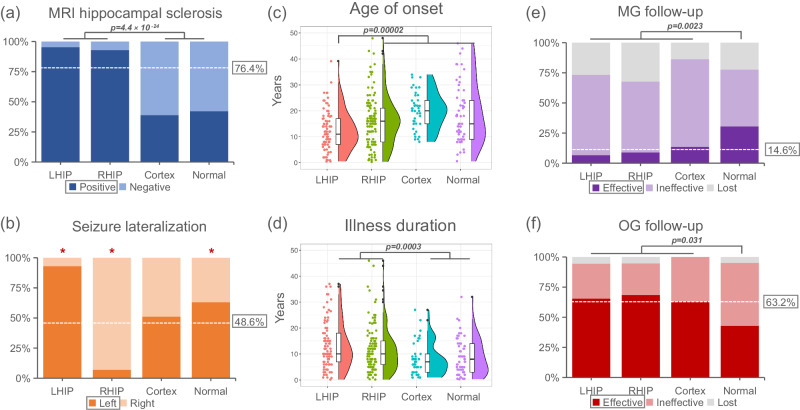
Artificial intelligence provides an opportunity to try to redefine disease subtypes based on similar pathobiology. Using a machine-learning algorithm (Subtype and Stage Inference) with cross-sectional MRI from 296 individuals with focal epilepsy originating from the temporal lobe (TLE) and 91 healthy controls, we show phenotypic heterogeneity in the pathophysiological progression of TLE. This study was registered in the Chinese Clinical Trials Registry (number: ChiCTR2200062562). We identify two hippocampus-predominant phenotypes, characterized by atrophy beginning in the left or right hippocampus; a third cortex-predominant phenotype, characterized by hippocampus atrophy after the neocortex; and a fourth phenotype without atrophy but amygdala enlargement. These four subtypes are replicated in the independent validation cohort (109 individuals). These subtypes show differences in neuroanatomical signature, disease progression and epilepsy characteristics. Five-year follow-up observations of these individuals reveal differential seizure outcomes among subtypes, indicating that specific subtypes may benefit from temporal surgery or pharmacological treatment. These findings suggest a diverse pathobiological basis underlying focal epilepsy that potentially yields to stratification and prognostication - a necessary step for precise medicine.
© 2024. The Author(s).
Conflict of interest statement
The author declares no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
