

Opioid use and subsequent delirium risk in patients with advanced cancer in palliative care: a multicenter registry study
- PMID: 38472471
- PMCID: PMC10933309
- DOI: 10.1038/s41598-024-56675-1
Opioid use and subsequent delirium risk in patients with advanced cancer in palliative care: a multicenter registry study
Abstract
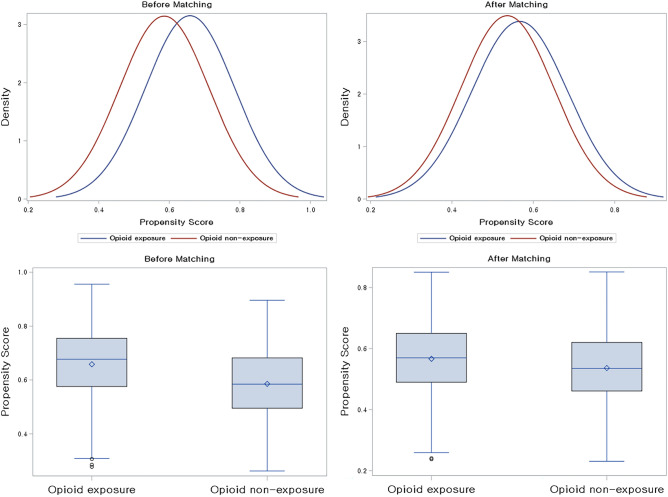
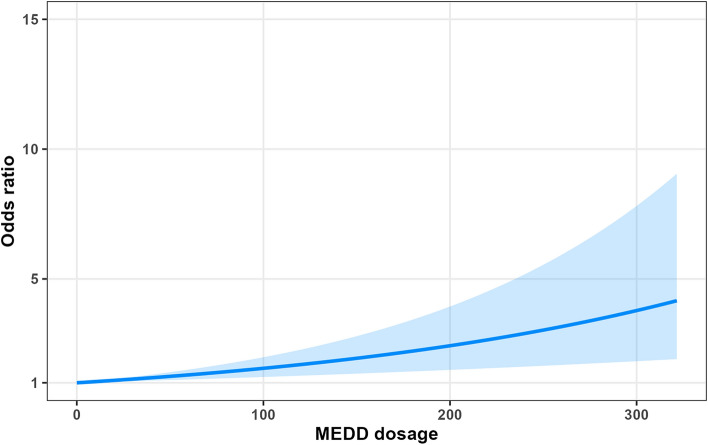
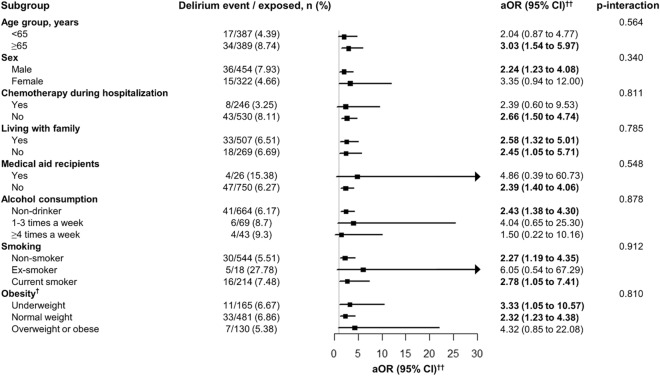
The prevalent use of opioids for pain management in patients with advanced cancer underscores the need for research on their neuropsychiatric impacts, particularly delirium. Therefore, we aimed to investigate the potential association between opioid use and the risk of delirium in patients with advanced cancer admitted to the acute palliative care unit. We conducted a retrospective observational study utilizing a multicenter, patient-based registry cohort by collecting the data from January 1, 2019, to December 31, 2020, in South Korea. All data regarding exposures, outcomes, and covariates were obtained through retrospective chart reviews by a team of specialized medical professionals with expertise in oncology. Full unmatched and 1:1 propensity-score matched cohorts were formed, and stratification analysis was conducted. The primary outcome, delirium, was defined and diagnosed by the DSM-IV. Of the 2,066 patients with advanced cancer, we identified 42.8% (mean [SD] age, 64.4 [13.3] years; 60.8% male) non-opioid users and 57.2% (62.8 [12.5] years; 55.9% male) opioid users, respectively. Opioid use was significantly associated with an increased occurrence of delirium in patients with advanced cancer (OR, 2.02 [95% CI 1.22-3.35]). The risk of delirium in patients with advanced cancer showed increasing trends in a dose-dependent manner. High-dose opioid users showed an increased risk of delirium in patients with advanced cancer compared to non-opioid users (low-dose user: OR, 2.21 [95% CI 1.27-3.84]; high-dose user: OR, 5.75 [95% CI 2.81-11.77]; ratio of OR, 2.60 [95% CI 1.05-6.44]). Patients with old age, male sex, absence of chemotherapy during hospitalization, and non-obese status were more susceptible to increased risk of delirium in patients with cancer. In this multicenter patient-based registry cohort study, we found a significant, dose-dependent association between opioid use and increased risk of delirium in patients with advanced cancer. We also identified specific patient groups more susceptible to delirium. These findings highlight the importance of opioid prescription in these patients with advanced cancer, balancing effective doses for pain management and adverse dose-inducing delirium.
Keywords: Cancer; Delirium; Opioid; Palliative care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
