

Case Reports
doi: 10.3390/diagnostics14050470.
Regression of Cardiac Rhabdomyomas Producing a Severe Aortic Stenosis: Case Report and Discussion of the Literature
Affiliations
- PMID: 38472942
- PMCID: PMC10930426
- DOI: 10.3390/diagnostics14050470
Item in Clipboard
Case Reports
Regression of Cardiac Rhabdomyomas Producing a Severe Aortic Stenosis: Case Report and Discussion of the Literature
Diagnostics (Basel).
.
Abstract
We describe a case of a voluminous rhabdomyoma (R) detected by fetal echocardiography at 32 weeks' gestation (w.g.) obstructing the left ventricular inflow and aortic outflow tract, with a moderate aortic gradient at birth, not needing immediate surgery. At follow-up, the mass progressively regressed, leaving the aortic valve partly damaged, with a gradient that increased to a maximum of 100 mmHg at 9 years. The girl was then operated on successfully by a plasty of the aortic valve. The literature regarding R is discussed.
Keywords: aortic stenosis; fetal echocardiography; fetus; rhabdomyoma.
Conflict of interest statement
The authors report no conflicts of interest.
Figures

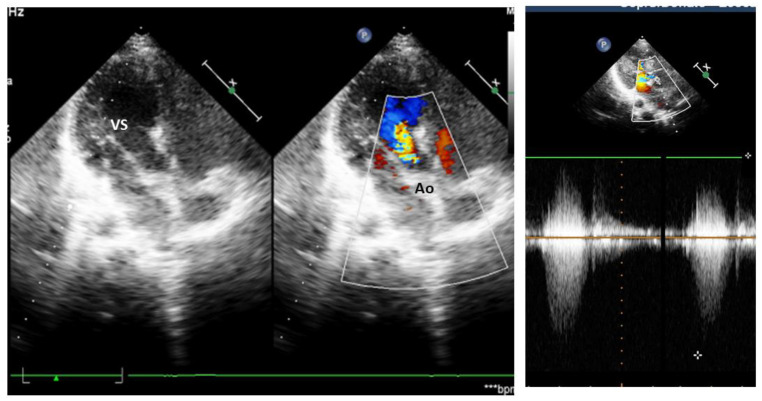
Fetal echocardiography at 32 w.g. A voluminous mass is evident in the left ventricle (VS) close to the inflow (a) and a smaller mass in the outflow toward the aorta (Ao) in the right panel (b). Color Doppler image is seen in panel (c) with a turbulent flow in aorta and pulsed Doppler of aorta in panel (d) with a max gradient of 200 cm/s at pulsed Doppler. VD—right ventricle.

Echocardiography at birth: both echodense masses are seen, with a turbulent aortic flow. Two masses are evident in the left ventricle (LV), a bigger one in the inflow, surrounded by a circle, and a smaller one in the aortic outflow tract (x). VS—left ventricle, Ao—aorta.
Echocardiography at 9 yrs. Only a small echodensity of a residual tumor is evident in the interventricular septum, with turbulent flow toward aorta, evident at color Doppler and with increased velocity at continuous wave Doppler at the right panel. (VS—left ventricle, ao—aorta).
References
Publication types
LinkOut - more resources
Full Text Sources
