

Pulmonary Biodistribution of Platelet-Derived Regenerative Exosomes in a Porcine Model
- PMID: 38473889
- PMCID: PMC10932369
- DOI: 10.3390/ijms25052642
Pulmonary Biodistribution of Platelet-Derived Regenerative Exosomes in a Porcine Model
Abstract
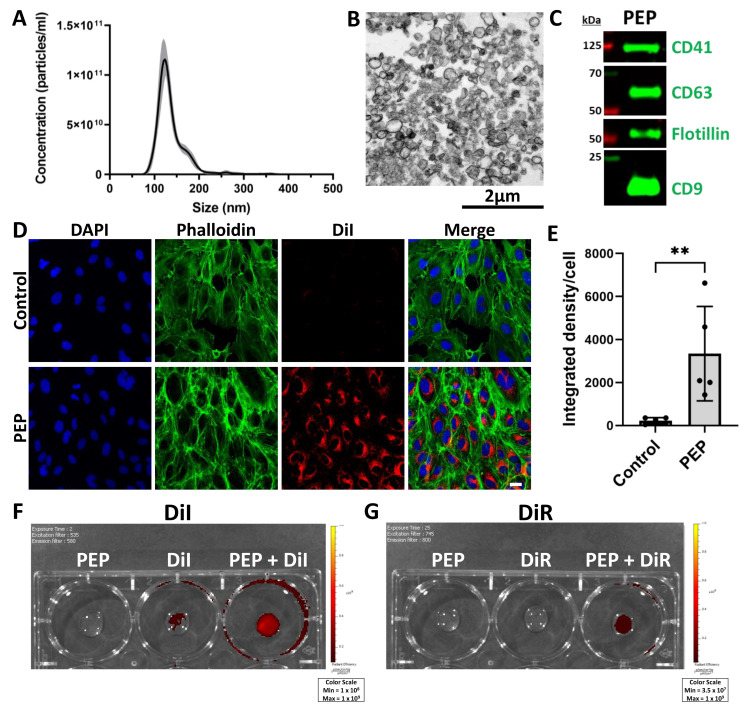
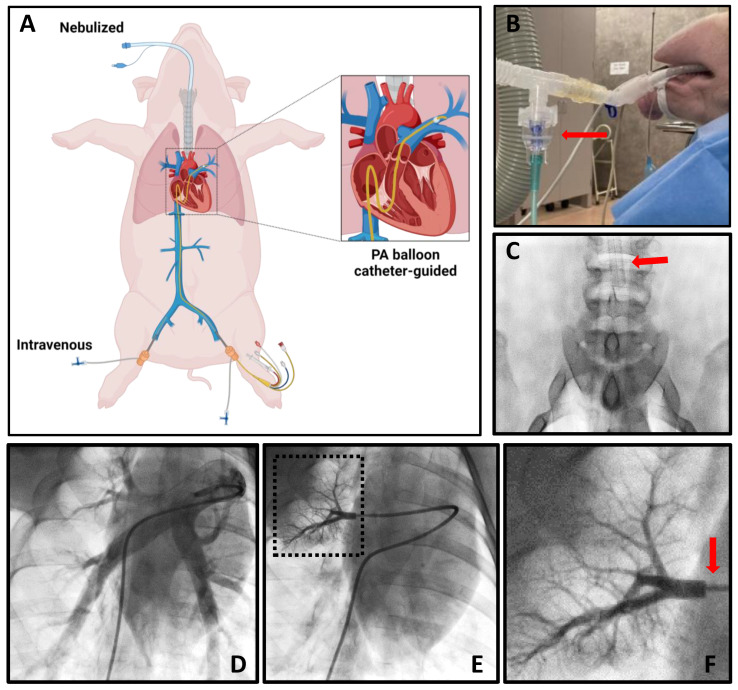
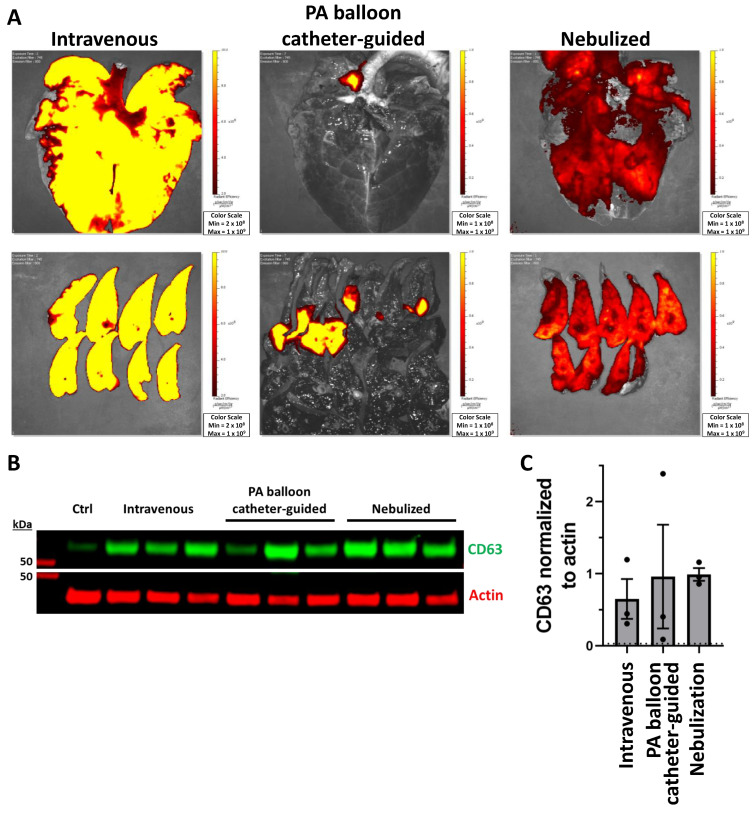
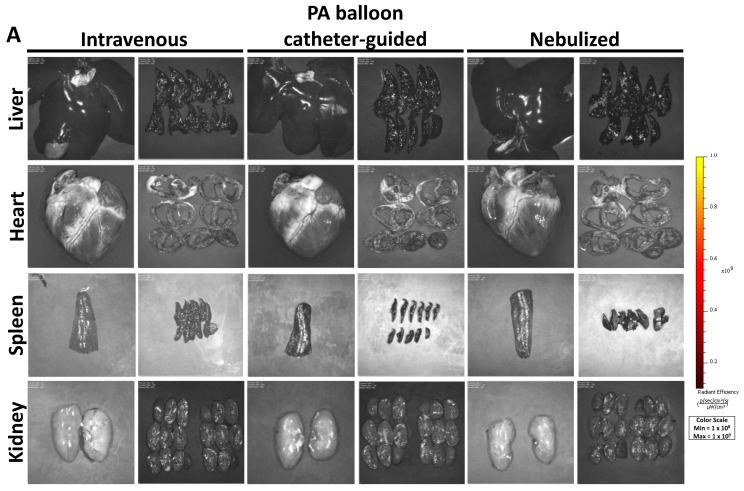
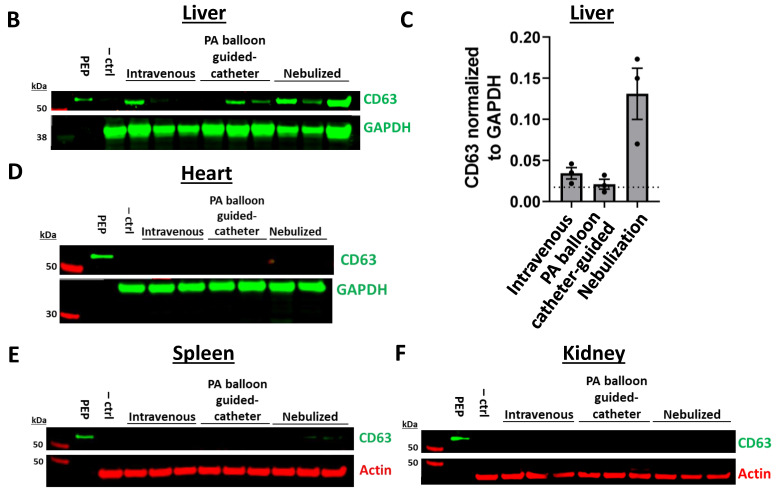
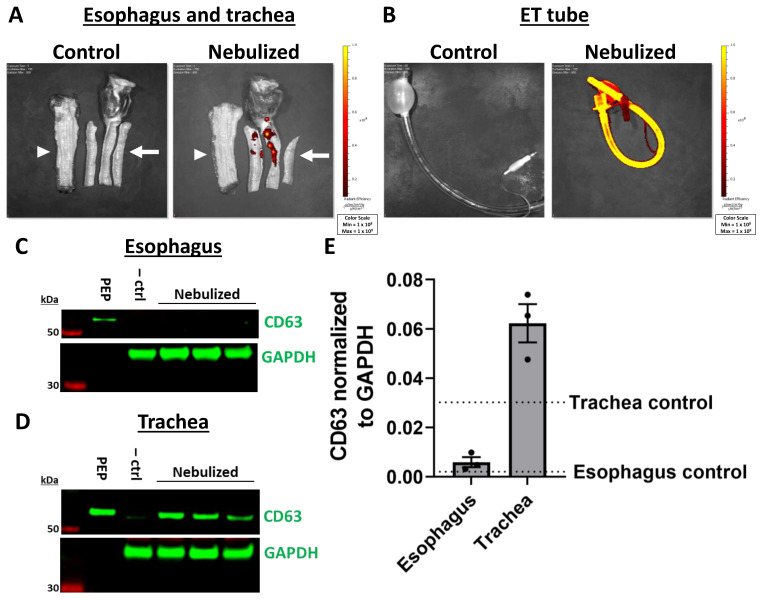
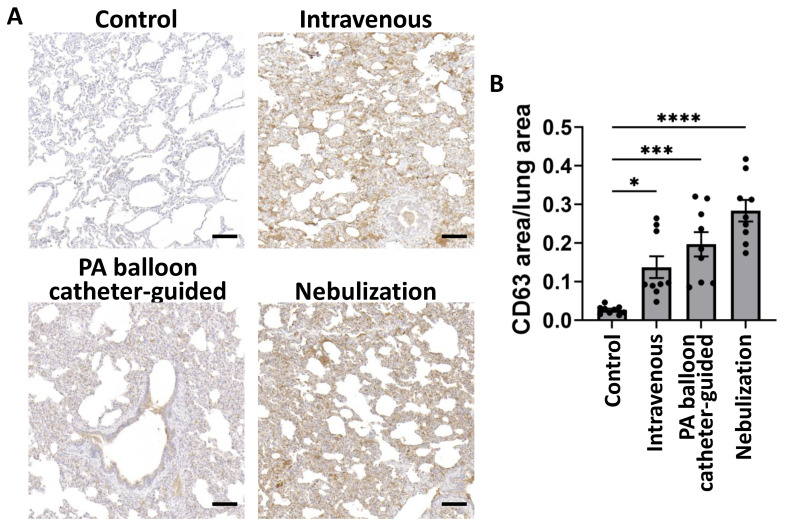
The purpose of this study was to evaluate the biodistribution of a platelet-derived exosome product (PEP), previously shown to promote regeneration in the setting of wound healing, in a porcine model delivered through various approaches. Exosomes were labeled with DiR far-red lipophilic dye to track and quantify exosomes in tissue, following delivery via intravenous, pulmonary artery balloon catheter, or nebulization in sus scrofa domestic pigs. Following euthanasia, far-red dye was detected by Xenogen IVUS imaging, while exosomal protein CD63 was detected by Western blot and immunohistochemistry. Nebulization and intravenous delivery both resulted in global uptake of exosomes within the lung parenchyma. However, nebulization resulted in the greatest degree of exosome uptake. Pulmonary artery balloon catheter-guided delivery provided the further ability to localize pulmonary delivery. No off-target absorption was noted in the heart, spleen, or kidney. However, the liver demonstrated uptake primarily in nebulization-treated animals. Nebulization also resulted in uptake in the trachea, without significant absorption in the esophagus. Overall, this study demonstrated the feasibility of pulmonary delivery of exosomes using nebulization or intravenous infusion to accomplish global delivery or pulmonary artery balloon catheter-guided delivery for localized delivery.
Keywords: biodistribution; exosomes; extracellular vesicles; pulmonary.
Conflict of interest statement
A.B. and P.G.S. and Mayo Clinic hold shares in Rion Inc. but have no other non-financial competing interests. All other authors declare no competing financial or non-financial interests.
Figures
References
-
- Wiklander O.P., Nordin J.Z., O’Loughlin A., Gustafsson Y., Corso G., Mager I., Vader P., Lee Y., Sork H., Seow Y., et al. Extracellular vesicle in vivo biodistribution is determined by cell source, route of administration and targeting. J. Extracell. Vesicles. 2015;4:26316. doi: 10.3402/jev.v4.26316. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
