

Nonintubated spontaneous ventilation versus intubated mechanical ventilation anesthesia for video-assisted thoracic surgery in terms of perioperative complications and practitioners' workload assessments: a pilot randomized control study
- PMID: 38475699
- PMCID: PMC10929236
- DOI: 10.1186/s12871-024-02481-1
Nonintubated spontaneous ventilation versus intubated mechanical ventilation anesthesia for video-assisted thoracic surgery in terms of perioperative complications and practitioners' workload assessments: a pilot randomized control study
Abstract
Background: The use of nonintubated video-assisted thoracoscopic surgery (NI-VATS) has been increasingly reported to yield favourable outcomes. However, this technology has not been routinely used because its advantages and safety have not been fully confirmed. The aim of this study was to assess the safety and feasibility of nonintubated spontaneous ventilation (NI-SV) anesthesia compared to intubated mechanical ventilation (I-MV) anesthesia in VATS by evaluating of perioperative complications and practitioners' workloads.
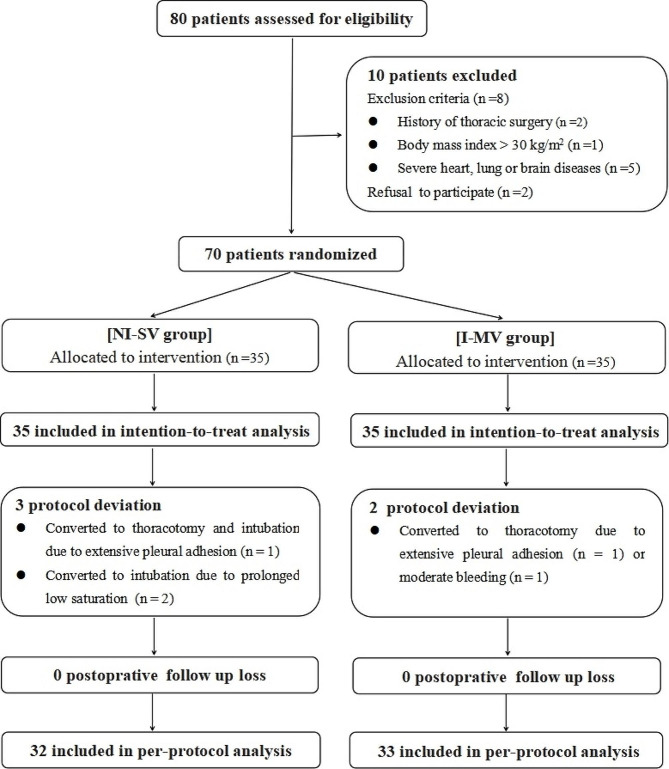
Methods: Patients who underwent uniportal VATS were randomly assigned at a 1:1 ratio to receive NI-SV or I-MV anesthesia. The primary outcome was the occurrence of intraoperative airway intervention events, including transient MV, conversion to intubation and repositioning of the double-lumen tube. The secondary outcomes included perioperative complications and modified National Aeronautics and Space Administration Task Load Index (NASA-TLX) scores from anesthesiologists and surgeons.
Results: Thirty-five patients in each group were enrolled in the intention-to-treat analysis. The incidence of intraoperative airway intervention events was greater in the NI-SV group than in the I-MV group (12 [34.3%] vs. 3 [8.6%]; OR = 0.180; 95% CI = 0.045-0.710; p = 0.009). No significant difference was found in the postoperative pulmonary complications between the groups (p > 0.05). The median of the anesthesiologists' overall NASA-TLX score was 37.5 (29-52) when administering the NI-SV, which was greater than the 25 (19-34.5) when the I-MV was administered (p < 0.001). The surgeons' overall NASA-TLX score was comparable between the two ventilation strategies (28 [21-38.5] vs. 27 [20.5-38.5], p = 0.814).
Conclusion: The NI-SV anesthesia was feasible for VATS in the selected patients, with a greater incidence of intraoperative airway intervention events than I-MV anesthesia, and with more surgical effort required by anesthesiologists.
Trial registration: Chinese Clinical Trial Registry, ChiCTR2200055427. https://www.chictr.org.cn/showproj.html?proj=147872 was registered on January 09, 2022.
Keywords: Intubation; Mechanical ventilation; Nonintubated; Spontaneous ventilation; Video-assisted thoracoscopic surgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Neto AS, Hemmes SN, Barbas CS, et al. Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data. Lancet Respir Med. 2016;4(4):272–80. doi: 10.1016/S2213-2600(16)00057-6. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
