

Transient but not chronic hyperglycemia accelerates ocular glymphatic transport
- PMID: 38475818
- PMCID: PMC10935920
- DOI: 10.1186/s12987-024-00524-w
Transient but not chronic hyperglycemia accelerates ocular glymphatic transport
Abstract
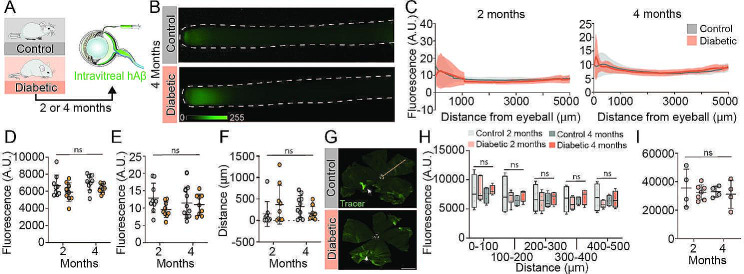
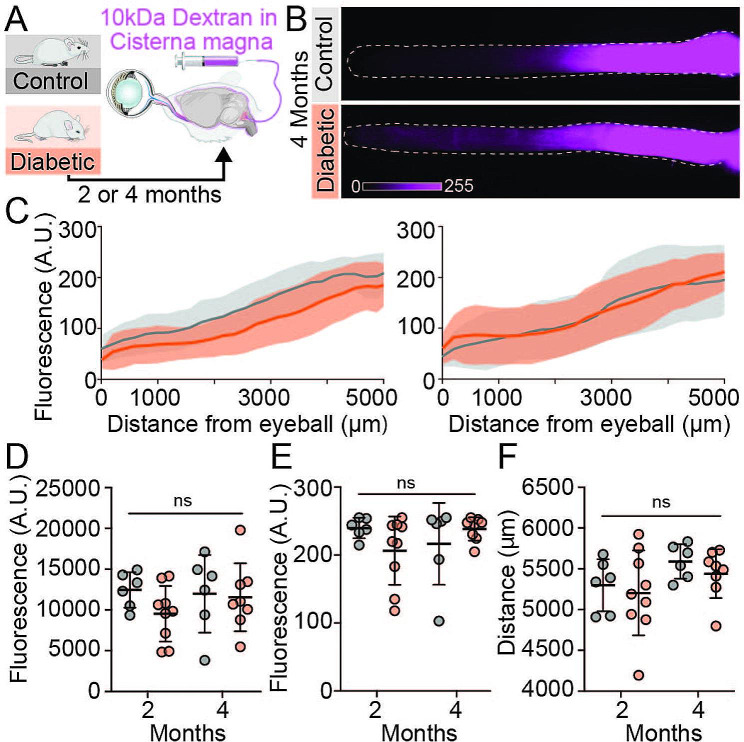
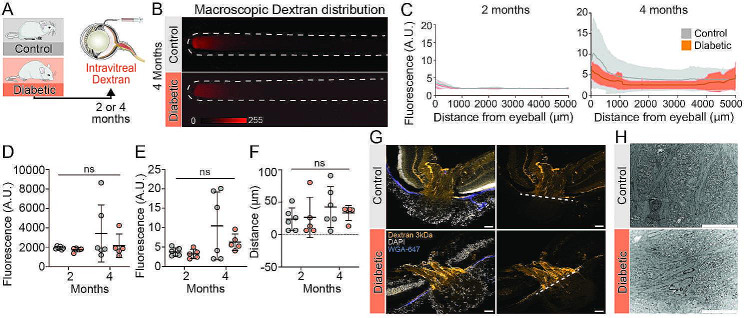
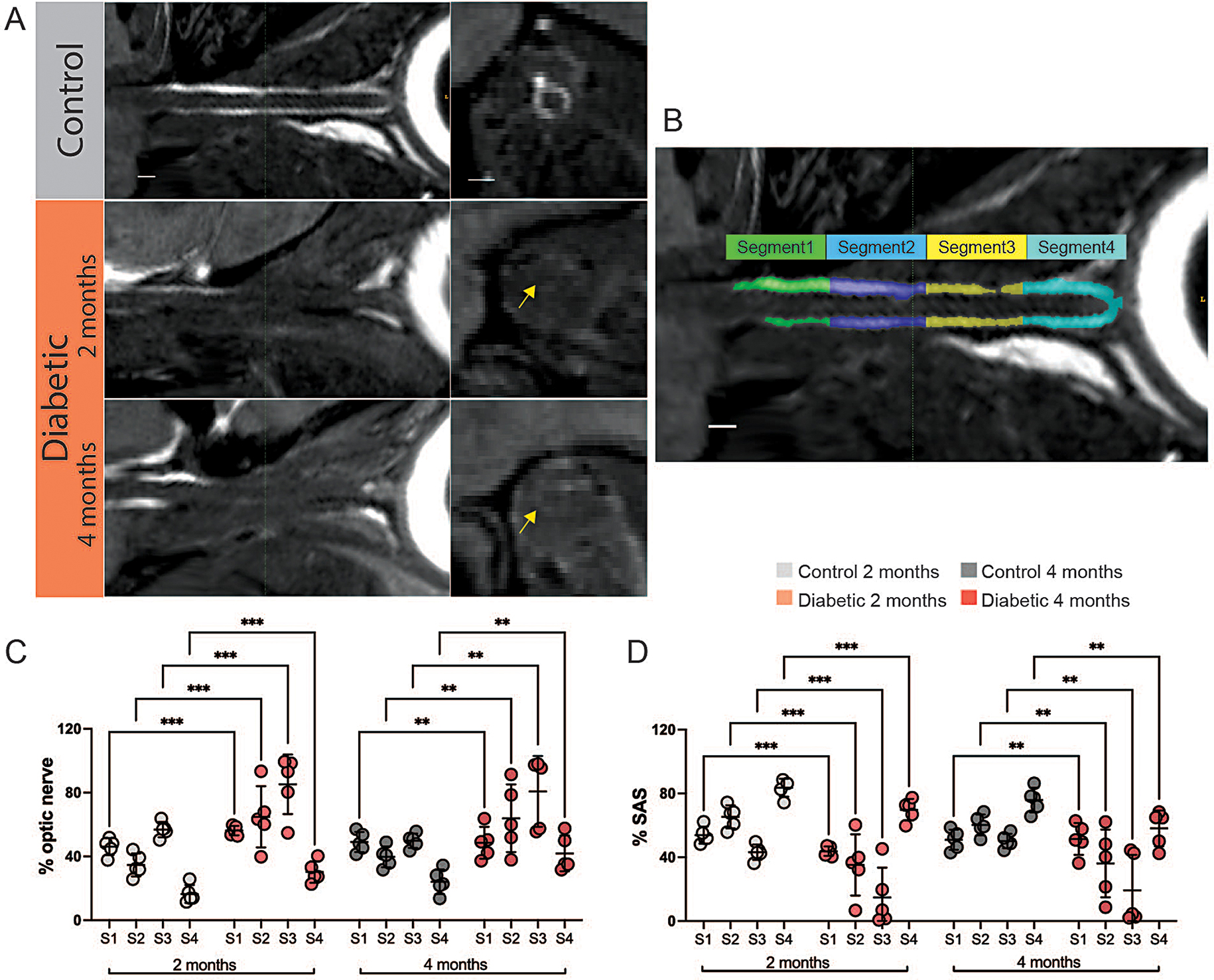
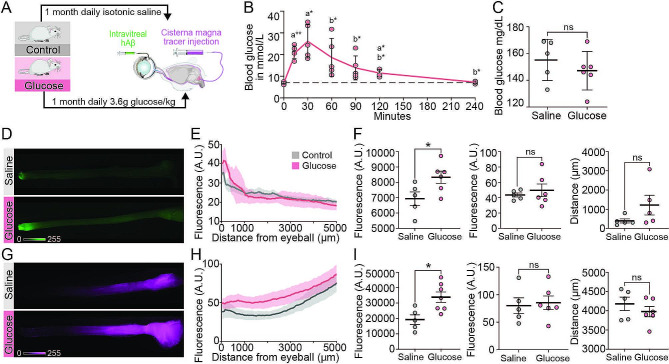
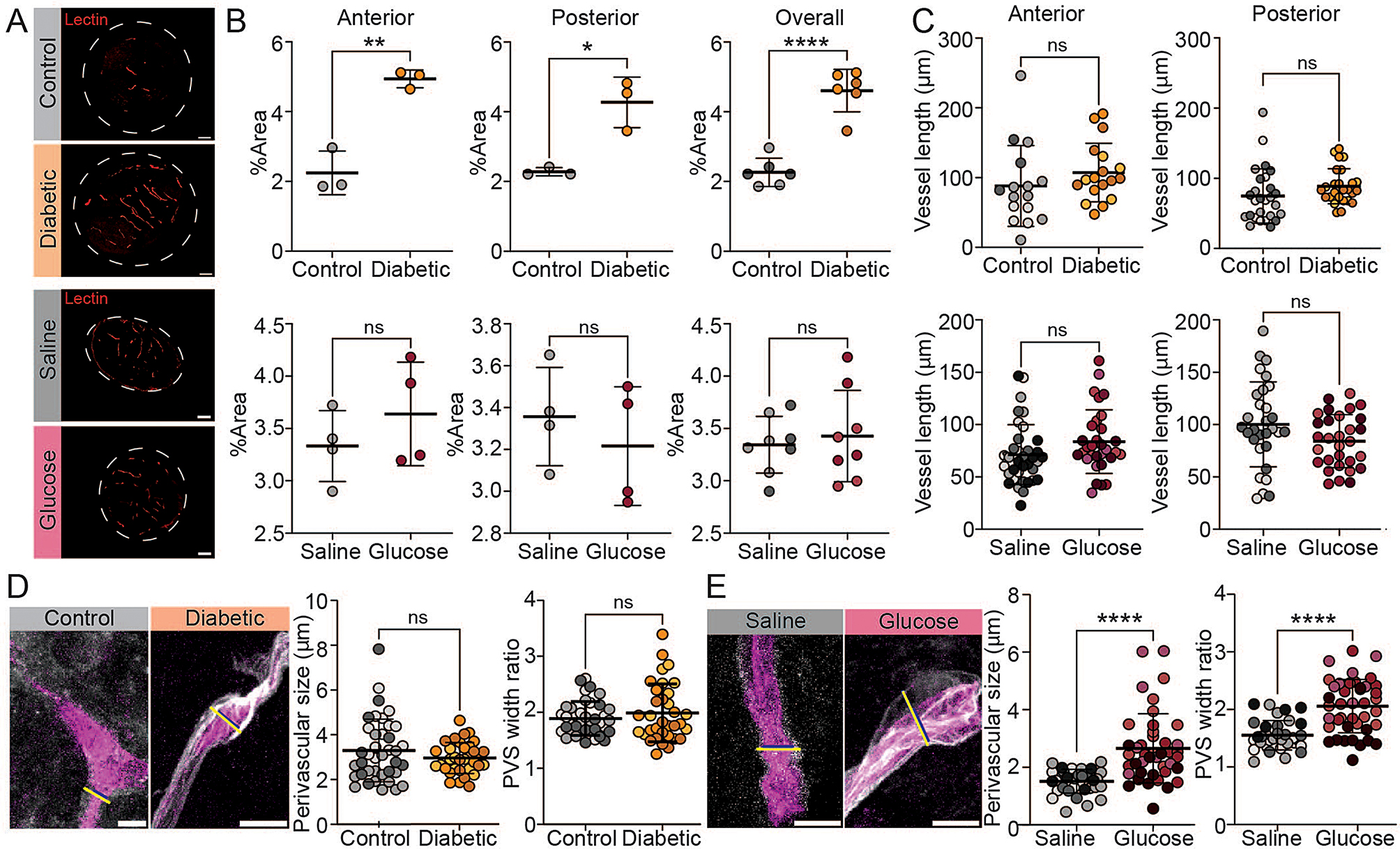
Glymphatic transport is vital for the physiological homeostasis of the retina and optic nerve. Pathological alterations of ocular glymphatic fluid transport and enlarged perivascular spaces have been described in glaucomatous mice. It remains to be established how diabetic retinopathy, which impairs vision in about 50% of diabetes patients, impacts ocular glymphatic fluid transport. Here, we examined ocular glymphatic transport in chronic hyperglycemic diabetic mice as well as in healthy mice experiencing a daily transient increase in blood glucose. Mice suffering from severe diabetes for two and four months, induced by streptozotocin, exhibited no alterations in ocular glymphatic fluid transport in the optic nerve compared to age-matched, non-diabetic controls. In contrast, transient increases in blood glucose induced by repeated daily glucose injections in healthy, awake, non-diabetic mice accelerated antero- and retrograde ocular glymphatic transport. Structural analysis showed enlarged perivascular spaces in the optic nerves of glucose-treated mice, which were absent in diabetic mice. Thus, transient repeated hyperglycemic events, but not constant hyperglycemia, ultimately enlarge perivascular spaces in the murine optic nerve. These findings indicate that fluid transport in the mouse eye is vulnerable to fluctuating glycemic levels rather than constant hyperglycemia, suggesting that poor glycemic control drives glymphatic malfunction and perivascular enlargement in the optic nerve.
Keywords: Cerebrospinal fluid; Diabetes; Glial lamina; Magnetic resonance imaging; Ocular glymphatic system; Perivascular spaces; Retina; Retinal ganglion cells; electron microscopy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The Ocular Glymphatic System-Current Understanding and Future Perspectives.Int J Mol Sci. 2024 May 24;25(11):5734. doi: 10.3390/ijms25115734. Int J Mol Sci. 2024. PMID: 38891923 Free PMC article. Review.
-
Does Long-Duration Exposure to Microgravity Lead to Dysregulation of the Brain and Ocular Glymphatic Systems?Eye Brain. 2022 May 4;14:49-58. doi: 10.2147/EB.S354710. eCollection 2022. Eye Brain. 2022. PMID: 35546965 Free PMC article. Review.
-
Degeneration of retinal ganglion cells in diabetic dogs and mice: relationship to glycemic control and retinal capillary degeneration.Mol Vis. 2013 Jun 27;19:1413-21. Print 2013. Mol Vis. 2013. PMID: 23825921 Free PMC article.
-
Glaucoma as a dangerous interplay between ocular fluid and cerebrospinal fluid.Med Hypotheses. 2019 Jun;127:97-99. doi: 10.1016/j.mehy.2019.04.008. Epub 2019 Apr 13. Med Hypotheses. 2019. PMID: 31088658
-
Metformin attenuated histopathological ocular deteriorations in a streptozotocin-induced hyperglycemic rat model.Naunyn Schmiedebergs Arch Pharmacol. 2021 Mar;394(3):457-467. doi: 10.1007/s00210-020-01989-w. Epub 2020 Oct 13. Naunyn Schmiedebergs Arch Pharmacol. 2021. PMID: 33047165
Cited by
-
Targeting oxidative stress in diabetic retinopathy: mechanisms, pathology, and novel treatment approaches.Front Immunol. 2025 Jun 16;16:1571576. doi: 10.3389/fimmu.2025.1571576. eCollection 2025. Front Immunol. 2025. PMID: 40589740 Free PMC article. Review.
-
Rewiring of the glymphatic landscape in metabolic disorders.Trends Endocrinol Metab. 2025 Aug;36(8):710-720. doi: 10.1016/j.tem.2024.11.005. Epub 2024 Dec 4. Trends Endocrinol Metab. 2025. PMID: 39638721 Review.
-
Loss of glymphatic homeostasis in heart failure.Brain. 2025 Mar 6;148(3):985-1000. doi: 10.1093/brain/awae411. Brain. 2025. PMID: 39693238 Free PMC article.
-
In vivo two-photon microscopy imaging of focused ultrasound-mediated glymphatic transport in the mouse brain.J Cereb Blood Flow Metab. 2025 Jul;45(7):1281-1292. doi: 10.1177/0271678X251323369. Epub 2025 Feb 22. J Cereb Blood Flow Metab. 2025. PMID: 39985197 Free PMC article.
-
The Ocular Glymphatic System-Current Understanding and Future Perspectives.Int J Mol Sci. 2024 May 24;25(11):5734. doi: 10.3390/ijms25115734. Int J Mol Sci. 2024. PMID: 38891923 Free PMC article. Review.
References
-
- Lee HJ, Seo HI, Cha HY, Yang YJ, Kwon SH, Yang SJ. Diabetes and Alzheimer’s Disease: Mechanisms and Nutritional Aspects. Clin Nutr Res [Internet]. 2018/10/23. 2018;7:229–40. Available from: https://pubmed.ncbi.nlm.nih.gov/30406052. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
