

Urinary markers of Mycobacterium tuberculosis and dysbiosis in paediatric tuberculous meningitis cases undergoing treatment
- PMID: 38475868
- PMCID: PMC10936073
- DOI: 10.1186/s13099-024-00609-9
Urinary markers of Mycobacterium tuberculosis and dysbiosis in paediatric tuberculous meningitis cases undergoing treatment
Abstract
Background: The pathogenesis of tuberculous meningitis (TBM) involves infection by Mycobacterium tuberculosis in the meninges and brain. However, recent studies have shown that the immune response and inflammatory processes triggered by TBM can have significant effects on gut microbiota. Disruptions in the gut microbiome have been linked to various systemic consequences, including altered immunity and metabolic dysregulation. Inflammation caused by TBM, antibiotic treatment, and changes in host immunity can all influence the composition of gut microbes. This complex relationship between TBM and the gut microbiome is of great importance in clinical settings. To gain a deeper understanding of the intricate interactions between TBM and the gut microbiome, we report innovative insights into the development of the disease in response to treatment. Ultimately, this could lead to improved outcomes, management strategies and quality of life for individuals affected by TBM.
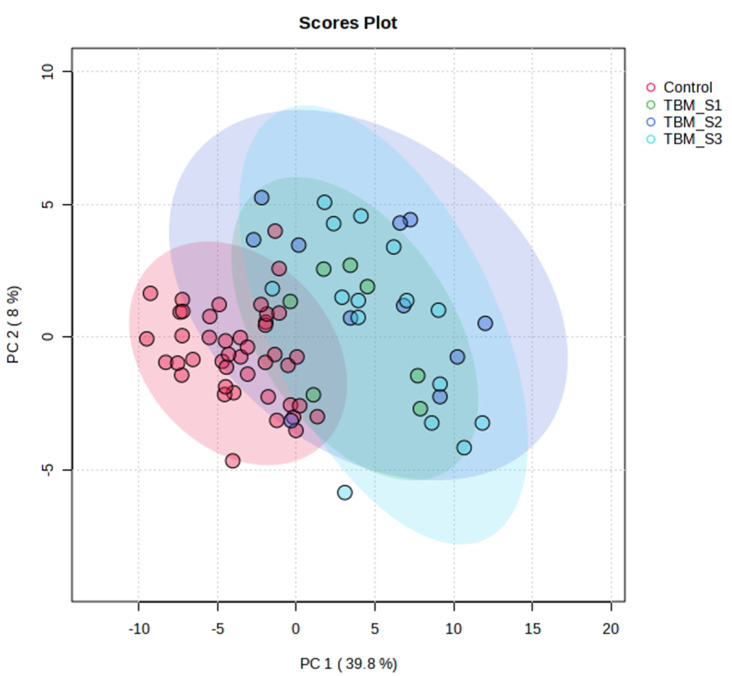
Method: We used a targeted liquid chromatography-tandem mass spectrometry (LC-MS/MS) approach to investigate metabolites associated with gut metabolism in paediatric participants by analysing the urine samples collected from a control group (n = 40), and an experimental group (n = 35) with confirmed TBM, which were subdivided into TBM stage 1 (n = 8), stage 2 (n = 11) and stage 3 (n = 16).
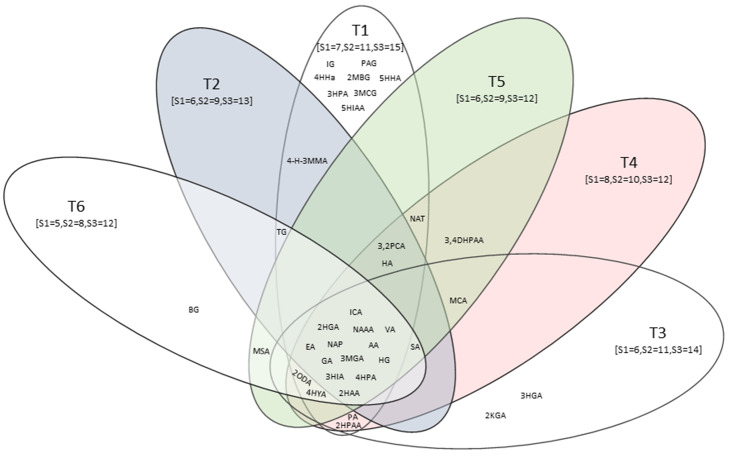
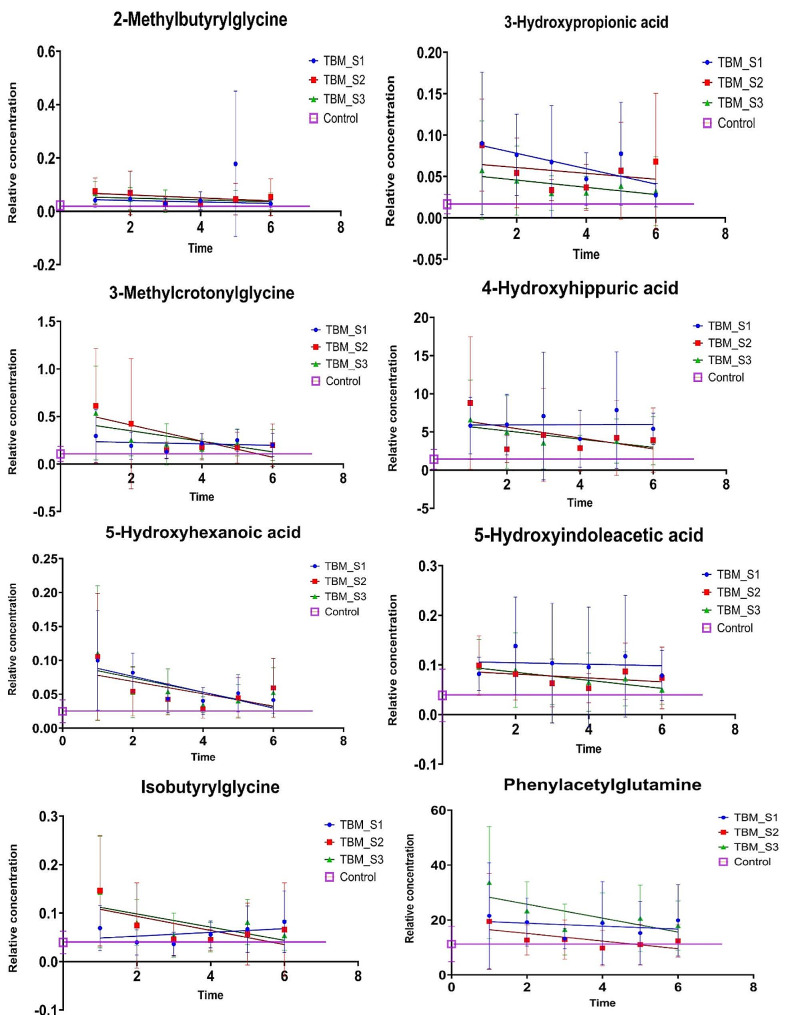
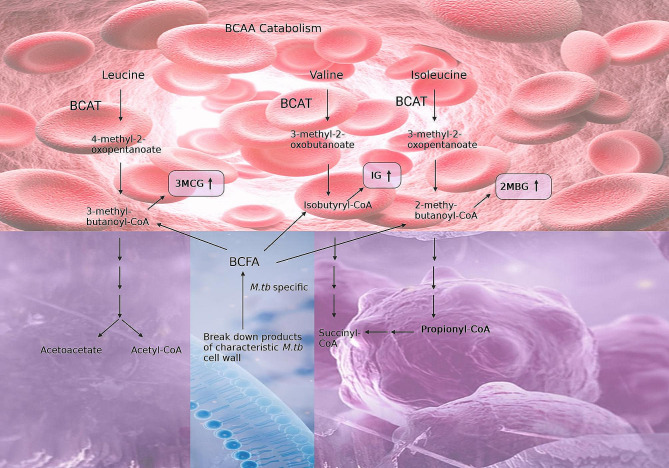
Findings: Our metabolomics investigation showed that, of the 78 initially selected compounds of microbiome origin, eight unique urinary metabolites were identified: 2-methylbutyrlglycine, 3-hydroxypropionic acid, 3-methylcrotonylglycine, 4-hydroxyhippuric acid, 5-hydroxyindoleacetic acid, 5-hydroxyhexanoic acid, isobutyrylglycine, and phenylacetylglutamine as urinary markers of dysbiosis in TBM.
Conclusion: These results - which are supported by previous urinary studies of tuberculosis - highlight the importance of gut metabolism and of identifying corresponding microbial metabolites as novel points for the foundation of improved management of TBM patients.
Keywords: Liquid chromatography-tandem mass spectrometry (LC-MS/MS); Metabolomics; Microbiota; Paediatric; Tuberculous meningitis (TBM); Urine.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
LinkOut - more resources
Full Text Sources
