

Human Fibroblast-Derived Matrix Hydrogel Accelerates Regenerative Wound Remodeling Through the Interactions with Macrophages
- PMID: 38476050
- PMCID: PMC11095160
- DOI: 10.1002/advs.202305852
Human Fibroblast-Derived Matrix Hydrogel Accelerates Regenerative Wound Remodeling Through the Interactions with Macrophages
Abstract
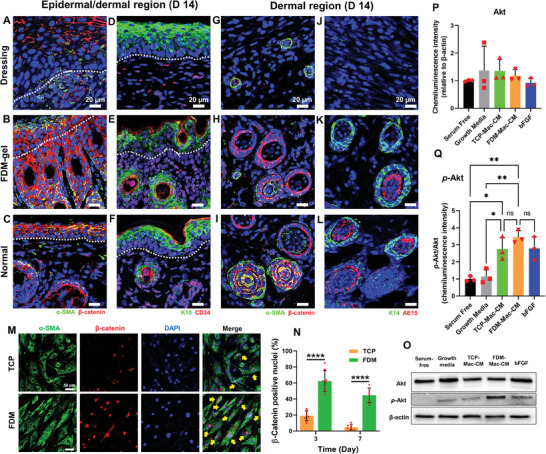
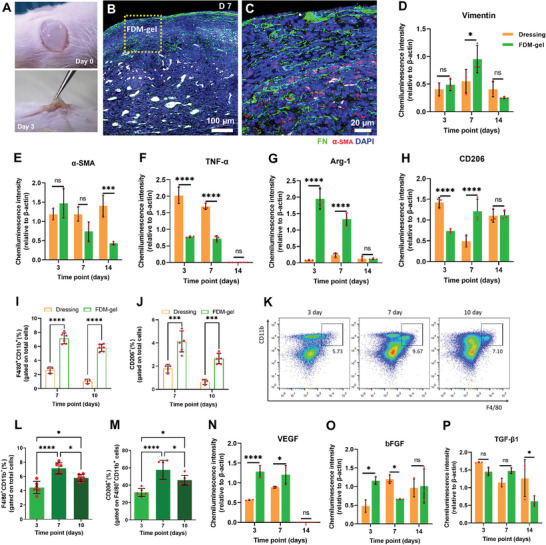
Herein, a novel extracellular matrix (ECM) hydrogel is proposed fabricated solely from decellularized, human fibroblast-derived matrix (FDM) toward advanced wound healing. This FDM-gel is physically very stable and viscoelastic, while preserving the natural ECM diversity and various bioactive factors. Subcutaneously transplanted FDM-gel provided a permissive environment for innate immune cells infiltration. Compared to collagen hydrogel, excellent wound healing indications of FDM-gel treated in the full-thickness wounds are noticed, particularly hair follicle formation via highly upregulated β-catenin. Sequential analysis of the regenerated wound tissues disclosed that FDM-gel significantly alleviated pro-inflammatory cytokine and promoted M2-like macrophages, along with significantly elevated vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) level. A mechanistic study demonstrated that macrophages-FDM interactions through cell surface integrins α5β1 and α1β1 resulted in significant production of VEGF and bFGF, increased Akt phosphorylation, and upregulated matrix metalloproteinase-9 activity. Interestingly, blocking such interactions using specific inhibitors (ATN161 for α5β1 and obtustatin for α1β1) negatively affected those pro-healing growth factors secretion. Macrophages depletion animal model significantly attenuated the healing effect of FDM-gel. This study demonstrates that the FDM-gel is an excellent immunomodulatory material that is permissive for host cells infiltration, resorbable with time, and interactive with macrophages, where it thus enables regenerative matrix remodeling toward a complete wound healing.
Keywords: cell‐derived, decellularized extracellular matrix; human fibroblast‐derived matrix hydrogel; macrophages; matrix‐macrophages interaction; wound healing.
© 2024 The Authors. Advanced Science published by Wiley‐VCH GmbH.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





Similar articles
-
Nano-Sized Extracellular Matrix Particles Lead to Therapeutic Improvement for Cutaneous Wound and Hindlimb Ischemia.Int J Mol Sci. 2021 Dec 9;22(24):13265. doi: 10.3390/ijms222413265. Int J Mol Sci. 2021. PMID: 34948061 Free PMC article.
-
Extracellular matrix/stromal vascular fraction gel conditioned medium accelerates wound healing in a murine model.Wound Repair Regen. 2017 Nov;25(6):923-932. doi: 10.1111/wrr.12602. Epub 2018 Feb 6. Wound Repair Regen. 2017. PMID: 29240284
-
Decellularized porcine dermal hydrogel enhances implant-based wound healing in the setting of irradiation.Acta Biomater. 2025 Jan 1;191:260-275. doi: 10.1016/j.actbio.2024.11.009. Epub 2024 Nov 8. Acta Biomater. 2025. PMID: 39522628
-
Implications of Extracellular Matrix Production by Adipose Tissue-Derived Stem Cells for Development of Wound Healing Therapies.Int J Mol Sci. 2017 May 31;18(6):1167. doi: 10.3390/ijms18061167. Int J Mol Sci. 2017. PMID: 28561757 Free PMC article. Review.
-
Rational Design of Immunomodulatory Hydrogels for Chronic Wound Healing.Adv Mater. 2021 Oct;33(39):e2100176. doi: 10.1002/adma.202100176. Epub 2021 Jul 12. Adv Mater. 2021. PMID: 34251690 Free PMC article. Review.
Cited by
-
Development of Biomaterials to Modulate the Function of Macrophages in Wound Healing.Bioengineering (Basel). 2024 Oct 12;11(10):1017. doi: 10.3390/bioengineering11101017. Bioengineering (Basel). 2024. PMID: 39451393 Free PMC article. Review.
-
Engineering cell-derived extracellular matrix for peripheral nerve regeneration.Mater Today Bio. 2024 Jun 13;27:101125. doi: 10.1016/j.mtbio.2024.101125. eCollection 2024 Aug. Mater Today Bio. 2024. PMID: 38979129 Free PMC article. Review.
-
Fibroblasts in heterotopic ossification: mechanisms and therapeutic targets.Int J Biol Sci. 2025 Jan 1;21(2):544-564. doi: 10.7150/ijbs.102297. eCollection 2025. Int J Biol Sci. 2025. PMID: 39781450 Free PMC article. Review.
-
A tactfully designed photothermal agent collaborating with ascorbic acid for boosting maxillofacial wound healing.Natl Sci Rev. 2024 Nov 26;12(2):nwae426. doi: 10.1093/nsr/nwae426. eCollection 2025 Feb. Natl Sci Rev. 2024. PMID: 39830404 Free PMC article.
-
Crosstalk Between H-Type Vascular Endothelial Cells and Macrophages: A Potential Regulator of Bone Homeostasis.J Inflamm Res. 2025 Feb 25;18:2743-2765. doi: 10.2147/JIR.S502604. eCollection 2025. J Inflamm Res. 2025. PMID: 40026304 Free PMC article. Review.
References
-
- Pomahač B., Svensjö T., Yao F., Brown H., Eriksson E., Crit. Rev. Oral Biol. Med. 1998, 9, 333. - PubMed
-
- Tan J., Luo G., Severe Trauma and Sepsis, Springer, New York: 2019, 345.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources