Short-segment percutaneous fusion versus open posterior fusion with screw in the fractured vertebra for thoracolumbar junction burst vertebral fracture treatment
- PMID: 38476412
- PMCID: PMC10927060
- DOI: 10.25259/JNRP_370_2023
Short-segment percutaneous fusion versus open posterior fusion with screw in the fractured vertebra for thoracolumbar junction burst vertebral fracture treatment
Abstract
Objectives: The treatment options for thoracolumbar junction burst fractures remain a topic of controversy. Short-segment percutaneous fixation (SSPF) and short-segment open fixation including the fractured level (SSOFIFL) are both viable procedures for managing these fractures. At present, there is a lack of evidence in the literature demonstrating the absolute superiority of one treatment over the other. This study aimed to compare these two surgical strategies with a focus on radiological and clinical outcomes.
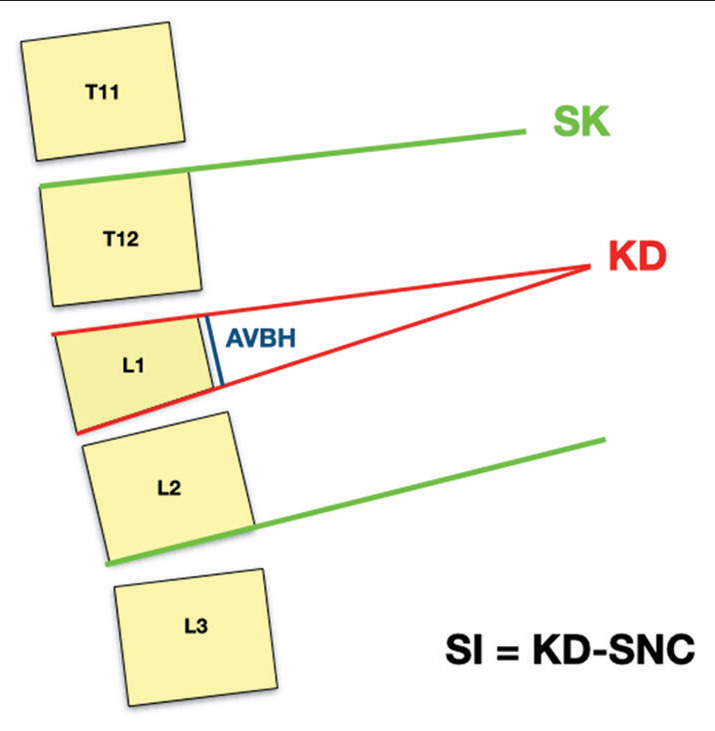
Materials and methods: This retrospective case-control multicenter analysis involved patients with A3 and A4 vertebral fractures at the thoracolumbar junction (T11-L2) who underwent surgical treatment with either SSPF or SSOFIFL in the participating centers. Clinical outcomes were measured using the Oswestry Disability Index and visual analogue scale (VAS) both pre- and postoperatively. Radiological outcomes included kyphotic deformity (KD), anterior vertebral body height (AVBH), segmental kyphosis, and sagittal alignment parameters.
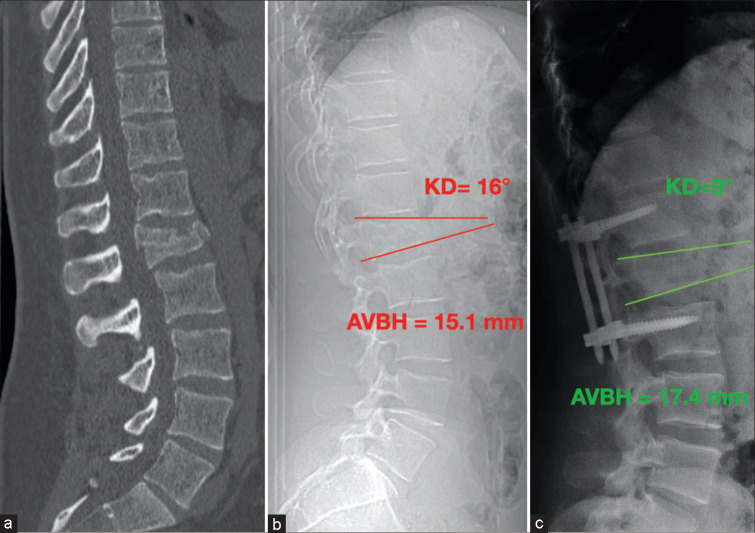
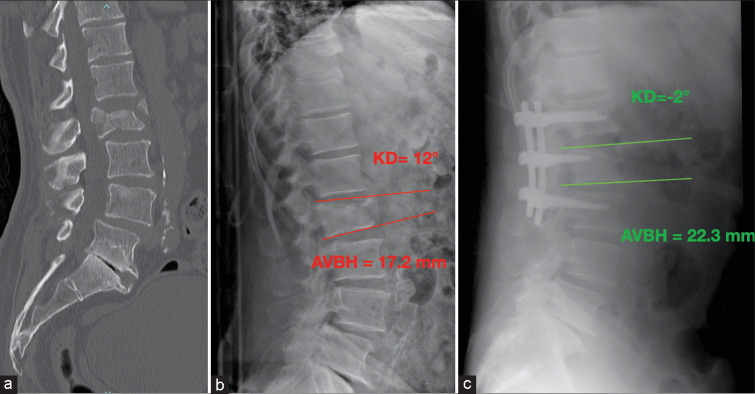
Results: A total of 156 patients were enrolled in the study, with 81 patients in Group A (SSPF) and 75 patients in Group B (SSOFIFL). Group B demonstrated better correction of KD (Group B: 3.4 ± 2.7° vs. Group A: 8.3 ± 3.2°, P = 0.003), AVBH, and sagittal alignment. A minor loss of correction was observed in Group B with respect to Group A (0.9 ± 1.7° vs 4.3° ± 2.1°, P = 0.043). Blood losses were lower in Group A (78 ± 15 min vs. 118 ± 23 min, P = 0.021) as well as during surgery (121.3 ± 34 mL vs. 210.2 ± 52 mL, P = 0.031), but the post-operative hemoglobin levels were comparable between the two groups.
Conclusion: SSOFIFL appears to show a major amount of KD correction and prevent loss of correction. This technique should be the preferred choice whenever possible. However, SSPF can be considered a valid alternative for damage control in polytrauma patients and fractures with low KD.
Keywords: Minimally invasive systems; Percutaneous pedicle screws; Short-segment fixation; Spinal surgery; Thoracolumbar burst fractures.
© 2024 Published by Scientific Scholar on behalf of Journal of Neurosciences in Rural Practice.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Comparison of short-segment pedicle fixation with versus without inclusion of the fracture level in the treatment of mild thoracolumbar burst fractures.Int J Surg. 2016 Dec;36(Pt A):352-357. doi: 10.1016/j.ijsu.2016.11.086. Epub 2016 Nov 17. Int J Surg. 2016. PMID: 27867025
-
Percutaneous pedicle screw fixation through the pedicle of fractured vertebra in the treatment of type A thoracolumbar fractures using Sextant system: an analysis of 38 cases.Chin J Traumatol. 2010 Jun 1;13(3):137-45. Chin J Traumatol. 2010. PMID: 20515590
-
Unipedicular-Screw Index Vertebra Manipulation Technique for Minimally Invasive Short-Segment Thoracolumbar Fracture Fixation.Int J Spine Surg. 2023 Oct;17(5):652-660. doi: 10.14444/8524. Epub 2023 Jul 24. Int J Spine Surg. 2023. PMID: 37487671 Free PMC article.
-
Treatment of unstable thoracolumbar junction fractures: short-segment pedicle fixation with inclusion of the fracture level versus long-segment instrumentation.Acta Neurochir (Wien). 2016 Oct;158(10):1883-9. doi: 10.1007/s00701-016-2907-0. Epub 2016 Aug 19. Acta Neurochir (Wien). 2016. PMID: 27541493
-
Kyphosis recurrence after posterior short-segment fixation in thoracolumbar burst fractures.J Neurosurg Spine. 2008 Mar;8(3):246-54. doi: 10.3171/SPI/2008/8/3/246. J Neurosurg Spine. 2008. PMID: 18312076
References
-
- Perna A, Santagada DA, Bocchi MB, Zirio G, Proietti L, Tamburrelli FC, et al. Early loss of angular kyphosis correction in patients with thoracolumbar vertebral burst (A3-A4) fractures who underwent percutaneous pedicle screws fixation. J Orthop. 2021;24:77–81. doi: 10.1016/j.jor.2021.02.029. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources