

Comparative risk of adverse perinatal outcomes associated with classes of antiretroviral therapy in pregnant women living with HIV: systematic review and meta-analysis
- PMID: 38476445
- PMCID: PMC10927998
- DOI: 10.3389/fmed.2024.1323813
Comparative risk of adverse perinatal outcomes associated with classes of antiretroviral therapy in pregnant women living with HIV: systematic review and meta-analysis
Abstract
Background: Integrase strand transfer inhibitor (INSTI) dolutegravir (DTG)-based antiretroviral therapy (ART) is recommended by World Health Organisation as preferred first-line regimen in pregnant women living with human immunodeficiency virus (HIV) (WLHIV). Non-nucleoside reverse transfer inhibitor (NNRTI)-based ART and protease inhibitor (PI)-based ART are designated as alternative regimens. The impact of different ART regimens on perinatal outcomes is uncertain. We aimed to assess the comparative risk of adverse perinatal outcomes in WLHIV receiving different classes of ART.
Materials and methods: A systematic literature review was conducted by searching PubMed, CINAHL, Global Health, and EMBASE for studies published between Jan 1, 1980, and July 14, 2023. We included studies reporting on the association of pregnant WLHIV receiving different classes of ART with 11 perinatal outcomes: preterm birth (PTB), very PTB, spontaneous PTB, low birthweight (LBW), very LBW, term LBW, preterm LBW, small for gestational age (SGA), very SGA (VSGA), stillbirth, and neonatal death. Pairwise random-effects meta-analyses compared the risk of each adverse perinatal outcome among WLHIV receiving INSTI-ART, NNRTI-ART, PI-ART, and nucleoside reverse transfer inhibitor (NRTI)-based ART, and compared specific "third drugs" from different ART classes. Subgroup and sensitivity analyses were conducted based on country income status and study quality.
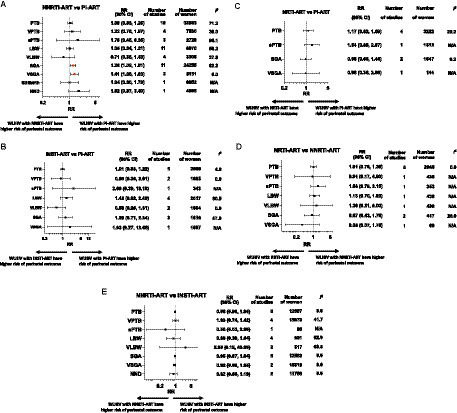
Results: Thirty cohort studies published in 2006-2022, including 222,312 pregnant women, met the eligibility criteria. Random-effects meta-analyses found no evidence that INSTI-ART is associated with adverse perinatal outcomes compared to NNRTI-ART and PI-ART. We found that PI-ART is associated with a significantly increased risk of SGA (RR 1.28, 95% confidence interval (95% CI) [1.09, 1.51], p = 0.003) and VSGA (RR 1.41, 95% CI [1.08, 1.83], p = 0.011), compared to NNRTI-ART. Specifically, lopinavir/ritonavir (LPV/r) was associated with an increased risk of SGA (RR 1.40, 95% CI [1.18, 1.65], p = 0.003) and VSGA (RR 1.84, 95% CI [1.37, 2.45], p = 0.002), compared to efavirenz, but not compared to nevirapine. We found no evidence that any class of ART or specific "third drug" was associated with an increased risk of PTB.
Conclusion: Our findings support the recommendation of INSTI-ART as first-line ART regimen for use in pregnant WLHIV. However, the increased risks of SGA and VGSA associated with PI-ART, compared to NNRTI-ART, may impact choice of second- and third-line ART regimens in pregnancy.Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42021248987.
Keywords: HIV; antiretroviral therapy; integrase inhibitor; low birthweight; perinatal outcome; preterm birth; protease inhibitor; small for gestational age.
Copyright © 2024 Beck, Cowdell, Portwood, Sexton, Kumarendran, Brandon, Kirtley and Hemelaar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Adverse perinatal outcomes associated with different classes of antiretroviral drugs in pregnant women with HIV.AIDS. 2025 Feb 1;39(2):162-174. doi: 10.1097/QAD.0000000000004032. Epub 2024 Oct 15. AIDS. 2025. PMID: 39407417 Free PMC article.
-
Adverse perinatal outcomes associated with protease inhibitor-based antiretroviral therapy in pregnant women living with HIV: A systematic review and meta-analysis.EClinicalMedicine. 2022 Apr 6;46:101368. doi: 10.1016/j.eclinm.2022.101368. eCollection 2022 Apr. EClinicalMedicine. 2022. PMID: 35521067 Free PMC article.
-
Adverse perinatal outcomes associated with antiretroviral therapy in women living with HIV: A systematic review and meta-analysis.Front Med (Lausanne). 2023 Feb 3;9:924593. doi: 10.3389/fmed.2022.924593. eCollection 2022. Front Med (Lausanne). 2023. PMID: 36816720 Free PMC article.
-
Adverse perinatal outcomes associated with prenatal exposure to protease-inhibitor-based versus non-nucleoside reverse transcriptase inhibitor-based antiretroviral combinations in pregnant women with HIV infection: a systematic review and meta-analysis.BMC Pregnancy Childbirth. 2023 Jan 30;23(1):80. doi: 10.1186/s12884-023-05347-5. BMC Pregnancy Childbirth. 2023. PMID: 36717801 Free PMC article.
-
Adverse perinatal outcomes associated with HAART and monotherapy.AIDS. 2022 Aug 1;36(10):1409-1427. doi: 10.1097/QAD.0000000000003248. Epub 2022 May 25. AIDS. 2022. PMID: 35608111
Cited by
-
Adverse perinatal outcomes associated with different classes of antiretroviral drugs in pregnant women with HIV.AIDS. 2025 Feb 1;39(2):162-174. doi: 10.1097/QAD.0000000000004032. Epub 2024 Oct 15. AIDS. 2025. PMID: 39407417 Free PMC article.
-
The effect of dolutegravir on obstetrical outcomes among women living with HIV: A retrospective cohort study.J Obstet Gynaecol Res. 2025 Jun;51(6):e16349. doi: 10.1111/jog.16349. J Obstet Gynaecol Res. 2025. PMID: 40545832 Free PMC article.
-
Care of the Child Perinatally Exposed to Human Immunodeficiency Virus.Clin Perinatol. 2024 Dec;51(4):881-894. doi: 10.1016/j.clp.2024.08.011. Clin Perinatol. 2024. PMID: 39487026 Review.
-
Perinatal outcomes among pregnant women with HIV initiating antiretroviral therapy preconception and antenatally.AIDS. 2025 Apr 1;39(5):584-596. doi: 10.1097/QAD.0000000000004104. Epub 2025 Jan 9. AIDS. 2025. PMID: 39760703 Free PMC article.
-
Foetal growth in pregnant women with HIV.AIDS. 2025 Sep 1;39(11):1568-1579. doi: 10.1097/QAD.0000000000004294. Epub 2025 Jul 8. AIDS. 2025. PMID: 40629838 Free PMC article.
References
-
- UNAIDS . Global AIDS update. Geneva: UNAIDS (2023).
-
- Sharrow D, Hug L, You D, Alkema L, Black R, Cousens S, et al. . Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the UN inter-agency Group for Child Mortality Estimation. Lancet Glob Health. (2022) 10:e195–206. doi: 10.1016/S2214-109X(21)00515-5, PMID: - DOI - PMC - PubMed
-
- Perin J, Mulick A, Yeung D, Villavicencio F, Lopez G, Strong KL, et al. . Global, regional, and national causes of under-5 mortality in 2000-19: an updated systematic analysis with implications for the sustainable development goals. Lancet Child Adolesc Health. (2022) 6:106–15. doi: 10.1016/S2352-4642(21)00311-4, PMID: - DOI - PMC - PubMed
-
- Lee AC, Kozuki N, Cousens S, Stevens GA, Blencowe H, Silveira MF, et al. . Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21st standard: analysis of CHERG datasets. BMJ. (2017) 358:j3677. doi: 10.1136/bmj.j3677 - DOI - PMC - PubMed
-
- Lee AC, Katz J, Blencowe H, Cousens S, Kozuki N, Vogel JP, et al. . National and regional estimates of term and preterm babies born small for gestational age in 138 low-income and middle-income countries in 2010. Lancet Glob Health. (2013) 1:e26–36. doi: 10.1016/S2214-109X(13)70006-8, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous