

Short-term versus usual-term antibiotic treatment for uncomplicated Staphylococcus aureus bacteremia: a systematic review and meta-analysis
- PMID: 38476737
- PMCID: PMC10929032
- DOI: 10.1177/20499361241237615
Short-term versus usual-term antibiotic treatment for uncomplicated Staphylococcus aureus bacteremia: a systematic review and meta-analysis
Abstract
Introduction: Uncomplicated Staphylococcus aureus bacteremia remains a leading cause of morbidity and mortality in hospitalized patients. Current guidelines recommend a minimum of 14 days of treatment.
Objective: To evaluate the efficacy and safety of short versus usual antibiotic therapy in adults with uncomplicated S. aureus bacteremia (SAB).
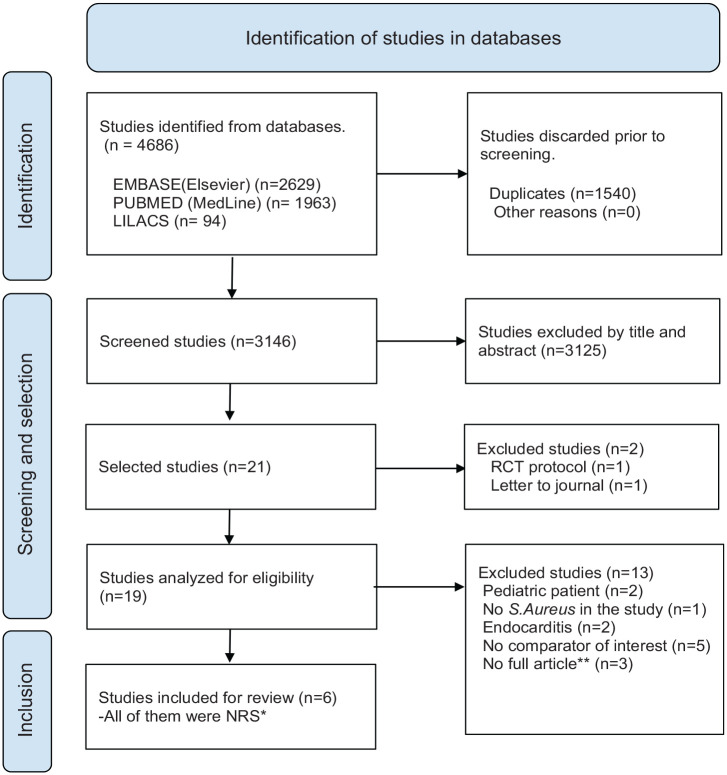
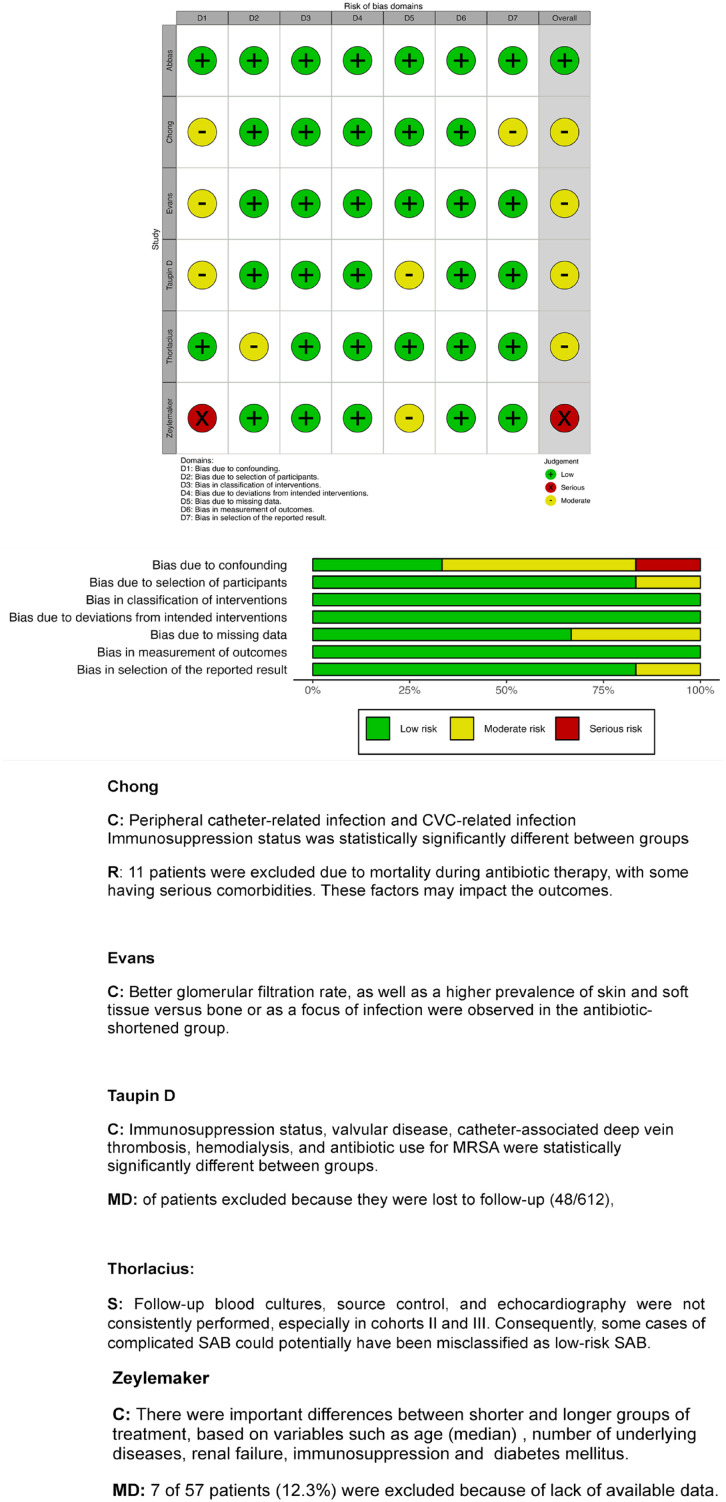
Methods: We developed a search strategy to identify systematic review and meta-analysis of non-randomized studies (NRS), comparing short versus usual or long antibiotic regimens for uncomplicated SAB in MEDLINE, Embase, and the Cochrane Register up to June 2023. The risk of bias was assessed using the ROBINS I tool. The meta-analysis was performed using Review Manager software with a random effect model.
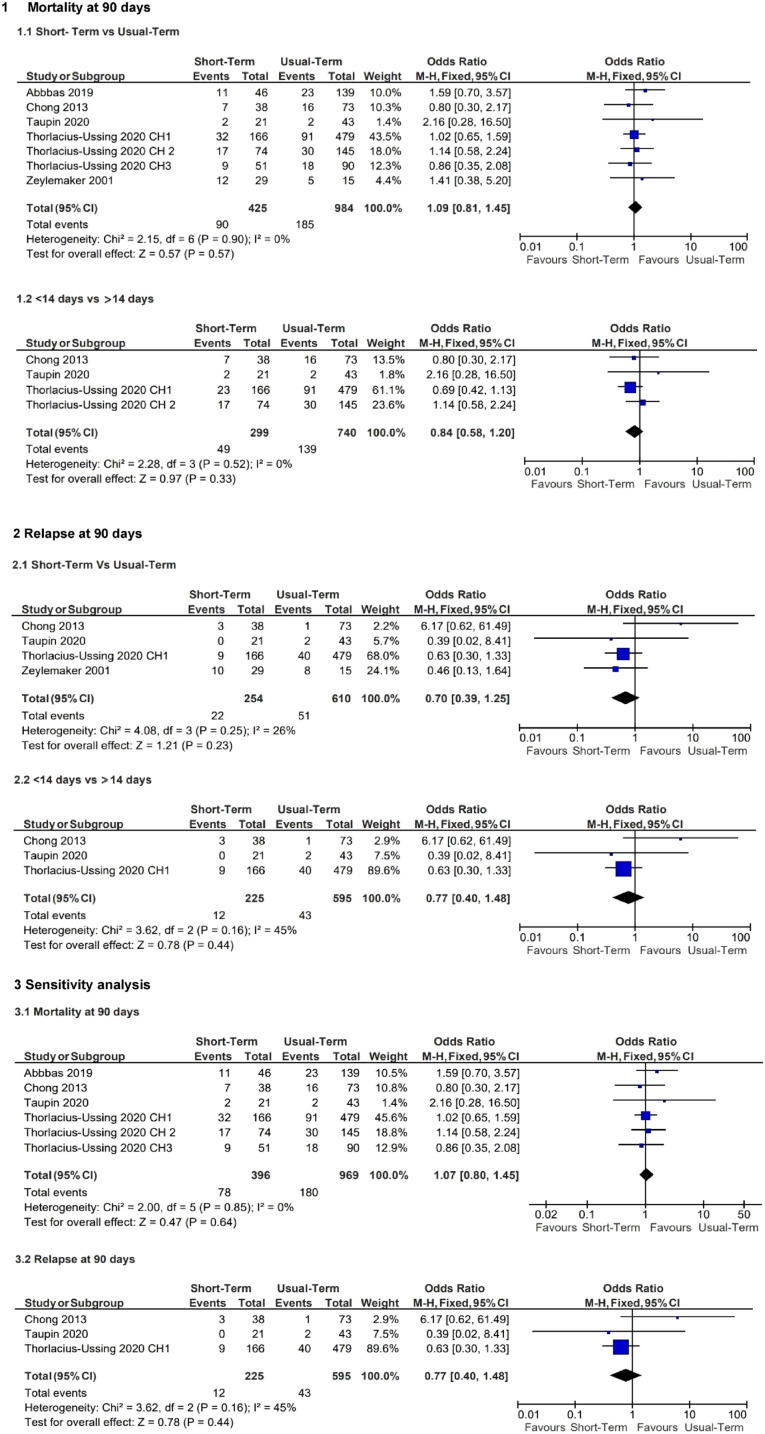
Results: Six NRS with a total of 1700 patients were included. No significant differences were found when comparing short versus prolonged antibiotic therapy as defined by the authors for 90-day mortality [odds ratio (OR): 1.09; 95% confidence interval (CI): 0.82-1.46, p: 0.55; I2 = 0%] or 90-day recurrence or relapse of bacteremia [OR: 0.72; 95% CI: 0.31-1.68, p: 0.45; I2 = 26%]. Sensitivity analysis showed similar results when comparing a predefined duration of <14 days versus ⩾14 days and when excluding the only study with a high risk of bias.
Conclusion: Shorter-duration regimens could be considered as an alternative option for uncomplicated SAB in low-risk cases. However, based on a small number of studies with significant methodological limitations and risk of bias, the benefits and harms of shorter regimens should be analyzed with caution. Randomized clinical trials are needed to determine the best approach regarding the optimal duration of therapy.
Keywords: Staphylococcus aureus; antibiotic duration; bacteremia; meta-analysis; systematic review.
Plain language summary
Comparing short and regular antibiotic treatment duration, for a type of blood infection caused by S. aureus We investigated the optimal duration of antibiotic treatment for adults with a specific type of blood infection (uncomplicated Staphylococcus aureus), a condition with a significant global impact on mortality and costs. After a thorough search, only six trials involving 1700 patients were identified. We therefore decided to perform a meta-analysis (a type of statistical analysis). The results showed that the duration of antibiotics, whether short or long (less or more than 14 days), did not significantly affect mortality or recurrence of infection within 90 days. Consequently, we suggested that shorter courses of antibiotics might be appropriate for less severe cases. However, we emphasized caution because of the limitations of the studies. We recommended further research with improved methods to determine the optimal approach to treating this type of infection.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Efficacy of seven and fourteen days of antibiotic treatment in uncomplicated Staphylococcus aureus bacteremia (SAB7): study protocol for a randomized controlled trial.Trials. 2019 May 2;20(1):250. doi: 10.1186/s13063-019-3357-9. Trials. 2019. PMID: 31046810 Free PMC article.
-
Long versus short course anti-microbial therapy of uncomplicated Staphylococcus aureus bacteraemia: a systematic review.Clin Microbiol Infect. 2024 Oct;30(10):1254-1260. doi: 10.1016/j.cmi.2024.05.015. Epub 2024 May 30. Clin Microbiol Infect. 2024. PMID: 38823452
-
Short-course versus long-course antibiotic treatment in patients with uncomplicated gram-negative bacteremia: A systematic review and meta-analysis.J Clin Pharm Ther. 2021 Feb;46(1):173-180. doi: 10.1111/jcpt.13277. Epub 2020 Sep 27. J Clin Pharm Ther. 2021. PMID: 32981149 Free PMC article.
-
Treatment duration for uncomplicated Staphylococcus aureus bacteremia to prevent relapse: analysis of a prospective observational cohort study.Antimicrob Agents Chemother. 2013 Mar;57(3):1150-6. doi: 10.1128/AAC.01021-12. Epub 2012 Dec 17. Antimicrob Agents Chemother. 2013. PMID: 23254436 Free PMC article.
-
Interventions to reduce Staphylococcus aureus in the management of eczema.Cochrane Database Syst Rev. 2019 Oct 29;2019(10):CD003871. doi: 10.1002/14651858.CD003871.pub3. Cochrane Database Syst Rev. 2019. PMID: 31684694 Free PMC article.
Cited by
-
Clinical Outcomes of Oral Antibiotic Switch in Children with Staphylococcus aureus Bacteremia.Turk Arch Pediatr. 2024 Sep 2;59(5):469-475. doi: 10.5152/TurkArchPediatr.2024.24108. Turk Arch Pediatr. 2024. PMID: 39440396 Free PMC article.
References
-
- Cisterna R, Ezpeleta C, Sota M. Epidemiology of bacteremia and of nosocomial infections. Clinical Microbiology and Infection. 1997; 3: 209–213.
-
- Inagaki K, Lucar J, Blackshear C, et al.. Methicillin-susceptible and methicillin-resistant Staphylococcus aureus bacteremia: nationwide estimates of 30-day readmission, in-hospital mortality, length of stay, and cost in the United States. Clin Infect Dis 2019; 69: 2112–2118. - PubMed
-
- Thampi N, Showler A, Burry L, et al.. Multicenter study of health care cost of patients admitted to hospital with Staphylococcus aureus bacteremia: impact of length of stay and intensity of care. Am J Infect Control 2015; 43: 739–744. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
