

Efficacy and safety of transcranial direct current stimulation to the ipsilesional motor cortex in subacute stroke (NETS): a multicenter, randomized, double-blind, placebo-controlled trial
- PMID: 38476746
- PMCID: PMC10928272
- DOI: 10.1016/j.lanepe.2023.100825
Efficacy and safety of transcranial direct current stimulation to the ipsilesional motor cortex in subacute stroke (NETS): a multicenter, randomized, double-blind, placebo-controlled trial
Abstract
Background: Each year, five million people are left disabled after stroke. Upper-extremity (UE) dysfunction is a leading problem. Neuroplasticity can be enhanced by non-invasive brain stimulation (NIBS) but evidence from large, randomized multicenter trials is lacking. We aimed at demonstrating efficacy of NIBS to enhance motor recovery after ischemic stroke.
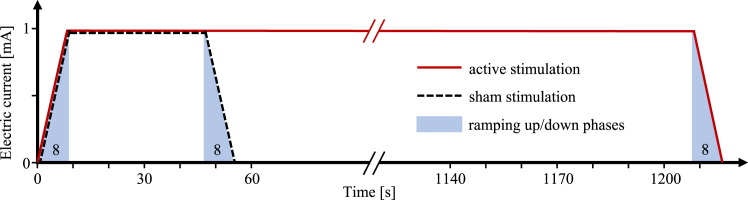
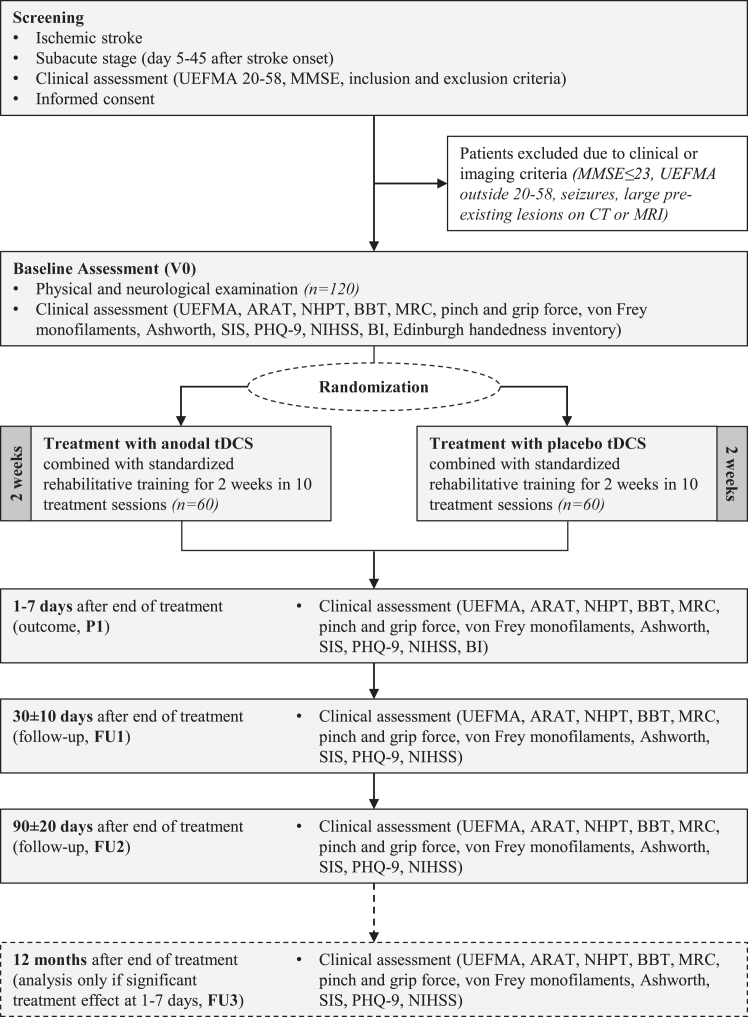
Methods: We randomly assigned patients to receive anodal transcranial direct current (tDCS, 1 mA, 20 min) or placebo stimulation ('control') over the primary motor cortex of the lesioned hemisphere in addition to standardized rehabilitative training over ten days in the subacute phase after stroke. The original study was planned to enrol 250 but, following a blinded interim analysis, ended with 123 participants. The primary outcome parameter was UE impairment, measured by UE-Fugl-Meyer-Assessment (UEFMA), one to seven days after the end of the treatment intervention (ClinicalTrials.gov, NCT00909714).
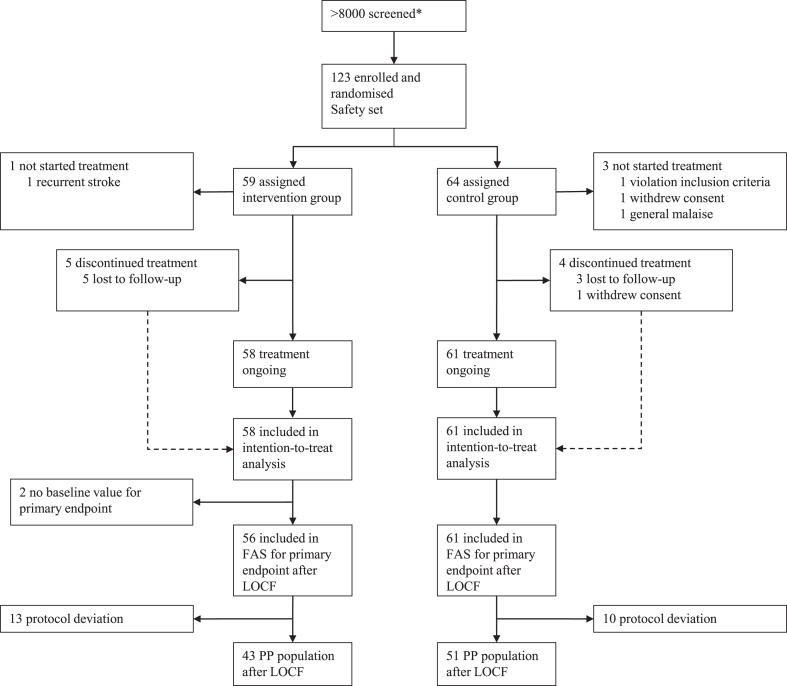
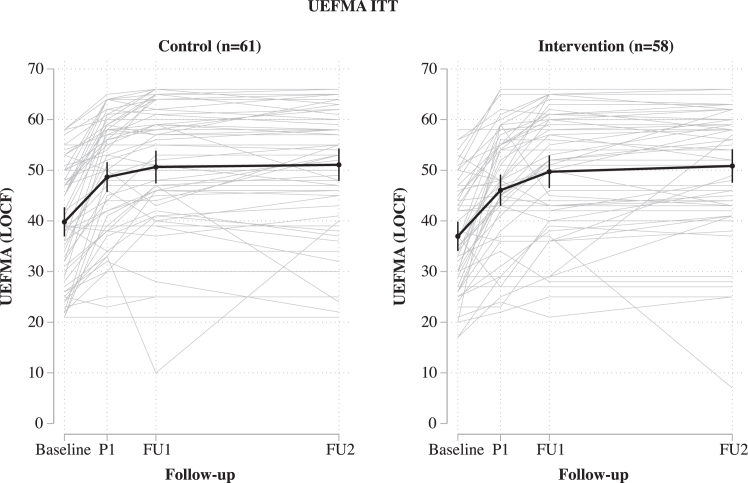
Findings: From 2009 to 2019, 123 patients were included, with 119 entering intention-to-treat analysis (ITT). The control group (N = 61) improved 8.9 (SD 7.7) UEFMA points, the tDCS group (N = 58) improved 9.0 (8.8) points. ITT was neutral with respect to the primary efficacy endpoint (p = 0.820). We found no difference in UEFMA change between active tDCS and control. The safety profile of tDCS was favorable. In particular, there were no seizures.
Interpretation: In patients with ischemic stroke, anodal tDCS applied to the motor cortex of the lesioned hemisphere over 10 days in the subacute phase was safe but did not improve the recovery of upper extremity function compared with placebo stimulation.
Funding: Deutsche Forschungsgemeinschaft (GE 844/4-1).
Keywords: Brain stimulation; Clinical trial; Neuroplasticity; Neurorehabilitation; Recovery; Stroke.
© 2023 The Author(s).
Conflict of interest statement
CG declares, independent of the presented study, grants from Deutsche Forschungsgemeinschaft (DFG), Deutsches Zentrum f. Luft-und Raumfahrt (DLR), Hertie Foundation, Wegener Foundation, Schilling Foundation, Werner Otto Foundation, Merz Pharmaceuticals, Allergan, European Union; CG declares consulting fees from AlphaSights Ltd., and Life Science Praxis S.L., honoraria (for lectures, presentations) from AstraZeneca GmbH, Elements Communications Ltd., Boehringer Ingelheim, Streamedup GmbH, Abbott Medical, Bayer AG; CG declares participation in the DSMB of RESSTORE1, work as an editor of INFO Neurologie & Psychiatrie, Therapie und Verlauf neurologischer Erkrankungen (Textbook), and membership of the presidium of the German Neurological Society (DGN). FCH declares, independent of the presented study, grants from EU, PHRT, SNSF, Bertarelli Foundation, Defitech Foundation, Wyss Center for Bio and Neuroengineering; FCH declares board membership of Novartis Foundation. KFH, SW, RS, and AZ declare no competing interests.
Figures
References
-
- Krakauer J.W. Motor learning: its relevance to stroke recovery and neurorehabilitation. Curr Opin Neurol. 2006;19:84–90. doi: 10.1097/01.wco.0000200544.29915.cc. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
