

Comparison of diagnostic performance of X‑ray, CT and MRI in patients with surgically confirmed subtle Lisfranc injuries
- PMID: 38476900
- PMCID: PMC10928826
- DOI: 10.3892/etm.2024.12462
Comparison of diagnostic performance of X‑ray, CT and MRI in patients with surgically confirmed subtle Lisfranc injuries
Abstract
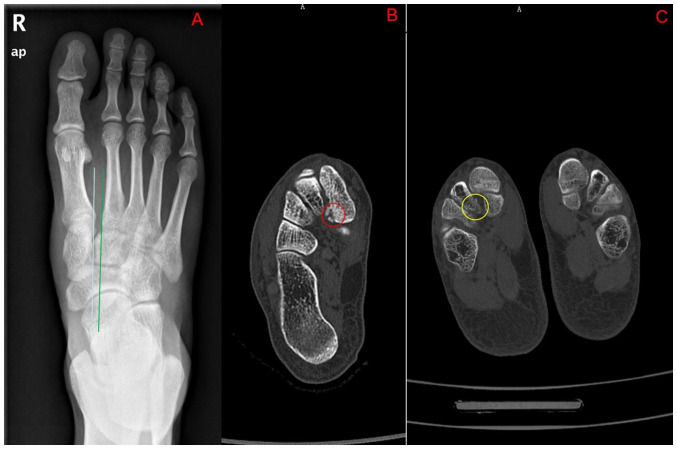
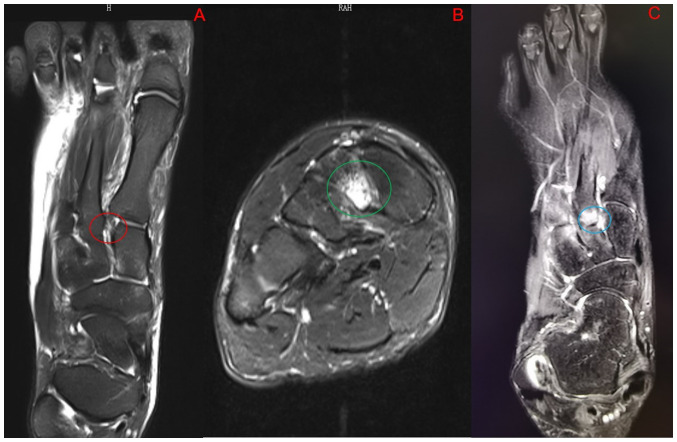
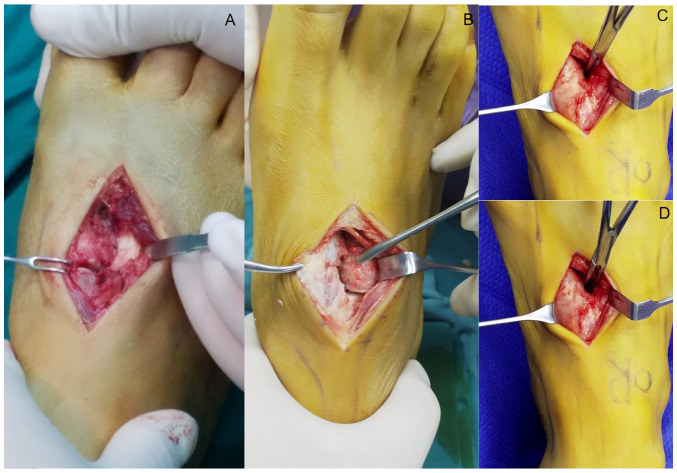
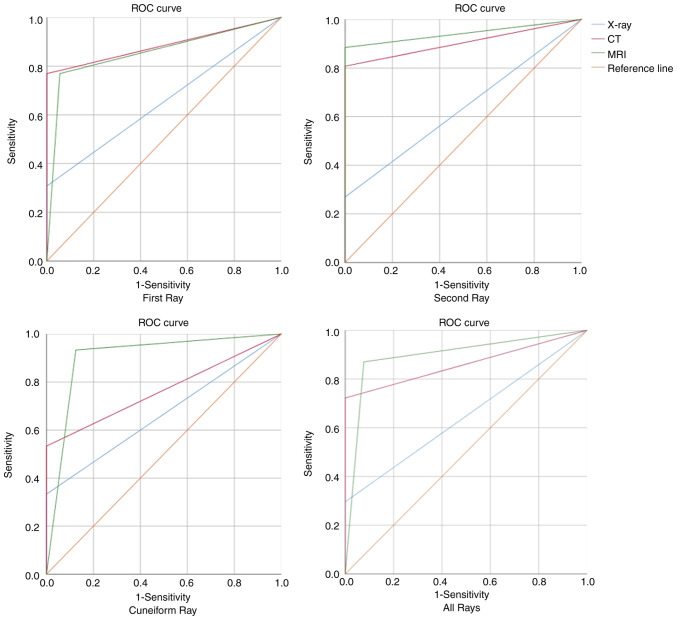
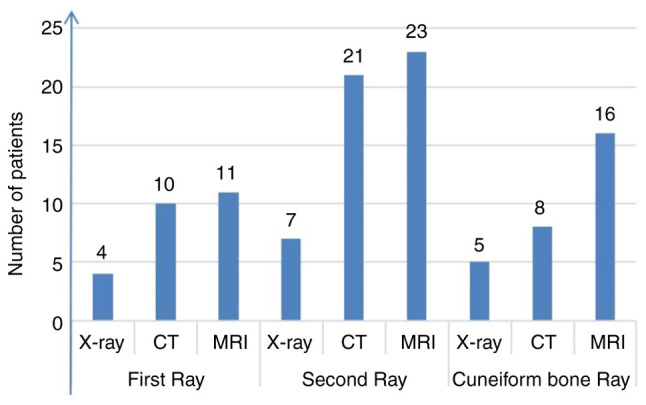
The present study aimed to compare the diagnostic performance of three imaging tests: X-ray, computed tomography (CT) and magnetic resonance imaging (MRI), for subtle Lisfranc injuries and three anatomical subtype injuries. The non-weight-bearing X-ray, CT and MRI imaging results of patients with subtle Lisfranc injuries from September 2013 to March 2022 were retrospectively reviewed. Subtle Lisfranc injuries and three anatomical subtypes (first, second and cuneiform rays) were diagnosed based on the surgical reports. The diagnostic performance of X-ray, CT and MRI was compared. The sensitivity (Sn), specificity (Sp), positive predictive value, negative predictive value, area under the receiver operating characteristic curve (AUC) and κ coefficient were reported. A total of 31 patients were included in the study. The correct diagnosis was made in 48.4% (15/31), 87.1% (27/31) and 96.8% (30/31) of patients by X-ray, CT and MRI, respectively. A total of 54 different anatomical injuries were found intraoperatively in all patients, with MRI and CT having high agreement (Sn, 72.2 and 87.0%; κ, 0.69 and 0.78, respectively) and X-ray having a low agreement (Sn, 29.6%; κ, 0.26) with the surgical findings. Regarding the first-ray injuries, CT had the highest Sn (76.9%), Sp (100%) and AUC (0.885) in diagnosing subtle Lisfranc injuries. MRI showed the best Sn (88.5 and 93.3%, respectively) and AUC (0.942 and 0.904, respectively) in both second and cuneiform rays. In conclusion, non-weight-bearing X-rays had poor diagnostic accuracy for subtle Lisfranc injuries and their subtypes. CT was superior to X-rays and MRI in diagnosing first-ray injuries. Although not significantly different from CT in terms of overall diagnosis, MRI was superior to X-ray and CT in diagnosing second and cuneiform-ray injuries.
Keywords: X-ray; computed tomography; imaging diagnosis; magnetic resonance imaging; subtle Lisfranc injury; tarsometatarsal joint.
Copyright: © 2024 Tang et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Weightbearing Computed Tomography Can Accurately Detect Subtle Lisfranc Injury.Foot Ankle Int. 2024 Oct;45(10):1145-1155. doi: 10.1177/10711007241266844. Epub 2024 Jul 30. Foot Ankle Int. 2024. PMID: 39080976
-
Weightbearing Computed Tomography vs Conventional Tomography for Examination of Varying Degrees of Lisfranc Injures: A Systematic Review of the Literature.Foot Ankle Orthop. 2023 Nov 23;8(4):24730114231209767. doi: 10.1177/24730114231209767. eCollection 2023 Oct. Foot Ankle Orthop. 2023. PMID: 38027457 Free PMC article.
-
Augmented Stress Weight-bearing CT for Evaluation of Subtle Lisfranc Injuries in the Elite Athlete.Foot Ankle Spec. 2024 Apr 3:19386400241241097. doi: 10.1177/19386400241241097. Online ahead of print. Foot Ankle Spec. 2024. PMID: 38567536
-
Imaging in Lisfranc injury: a systematic literature review.Skeletal Radiol. 2020 Jan;49(1):31-53. doi: 10.1007/s00256-019-03282-1. Epub 2019 Jul 31. Skeletal Radiol. 2020. PMID: 31368007
-
Diagnostic challenges of Lisfranc joint injuries: A review of imaging methods.Wiad Lek. 2025;78(3):626-633. doi: 10.36740/WLek/202333. Wiad Lek. 2025. PMID: 40219893 Review.
References
LinkOut - more resources
Full Text Sources