

Unilateral percutaneous vertebroplasty in osteoporotic vertebral compression fractures: A clinical efficacy evaluation
- PMID: 38476906
- PMCID: PMC10928977
- DOI: 10.3892/etm.2024.12439
Unilateral percutaneous vertebroplasty in osteoporotic vertebral compression fractures: A clinical efficacy evaluation
Abstract
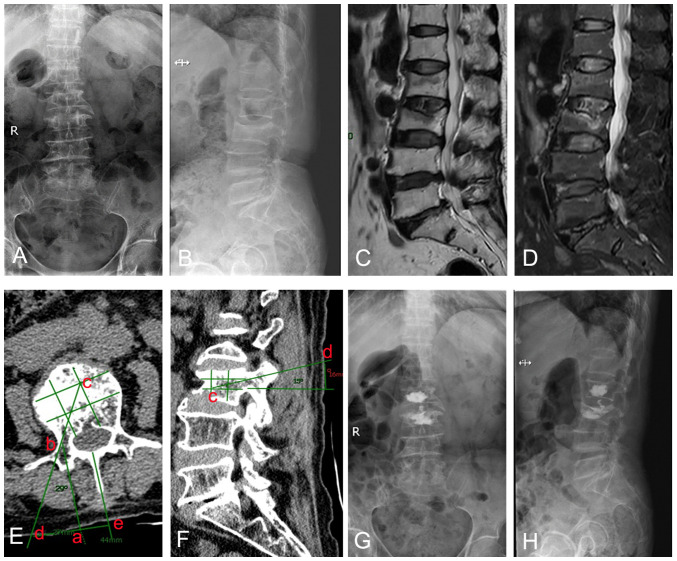
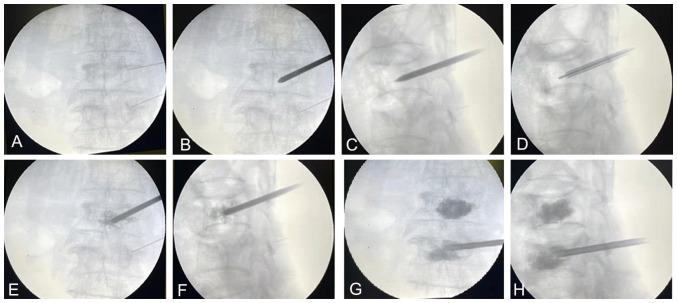
Osteoporotic vertebral compression fractures, often resulting from low-energy trauma, markedly impair the quality of life of elderly individuals. The present retrospective study focused on the clinical efficacy of unilateral percutaneous vertebroplasty (PVP) in the treatment of osteoporotic compression fractures. A total of 68 patients, representing 92 vertebral bodies, who underwent the unilateral PVP technique from March 2020 to January 2023 were evaluated. Key parameters such as visual analogue scale (VAS) values, Oswestry disability index (ODI) scores, Cobb angle measurements, and anterior vertebral height (AVH) were documented pre- and post-surgery. The mean follow-up period was 15.41±3.74 months. The mean pre-operative VAS score was 8.08±0.79, which was significantly reduced to 2.25±0.71 by 24 h post-surgery and stabilized at 1.58±0.51 by the final follow-up. The ODI showed a significant improvement from a pre-operative average of 67.75±7.91 to 19.74±2.90 post-surgery, and was maintained at a low level of 28.00±4.89 at the last assessment. Radiological evaluations revealed significant alterations in Cobb angle and AVH post-operation. Notably, during the follow-up, eight patients developed new compression fractures in different vertebral segments. In conclusion, the unilateral PVP method is safe and efficient for the management of osteoporotic vertebral compression fractures.
Keywords: elderly; osteoporotic fractures; quality of life; unilateral percutaneous vertebroplasty; vertebral compression fractures.
Copyright: © 2024 Shi et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Firanescu CE, de Vries J, Lodder P, Venmans A, Schoemaker MC, Smeets AJ, Donga E, Juttmann JR, Klazen CAH, Elgersma OEH, et al. Vertebroplasty versus sham procedure for painful acute osteoporotic vertebral compression fractures (VERTOS IV): Randomised sham controlled clinical trial. BMJ. 2018;361(k1551) doi: 10.1136/bmj.k1551. - DOI - PMC - PubMed
-
- Akesson K, Marsh D, Mitchell PJ, McLellan AR, Stenmark J, Pierroz DD, Kyer C, Cooper C. Capture the fracture: A best practice framework and global campaign to break the fragility fracture cycle. Osteoporos Int. 2013;24:2135–2152. doi: 10.1007/s00198-013-2348-z. IOF Fracture Working Group. - DOI - PMC - PubMed
-
- Voormolen MH, Lohle PN, Lampmann LE, van den Wildenberg W, Juttmann JR, Diekerhof CH, de Waal Malefijt J. Prospective clinical follow-up after percutaneous vertebroplasty in patients with painful osteoporotic vertebral compression fractures. J Vasc Interv Radiol. 2006;17:1313–1320. doi: 10.1097/01.RVI.0000231952.75209.4A. - DOI - PubMed
LinkOut - more resources
Full Text Sources