

Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
- PMID: 38476957
- PMCID: PMC10928809
- DOI: 10.1093/bjrai/ubae003
Artificial intelligence in medicine: mitigating risks and maximizing benefits via quality assurance, quality control, and acceptance testing
Abstract
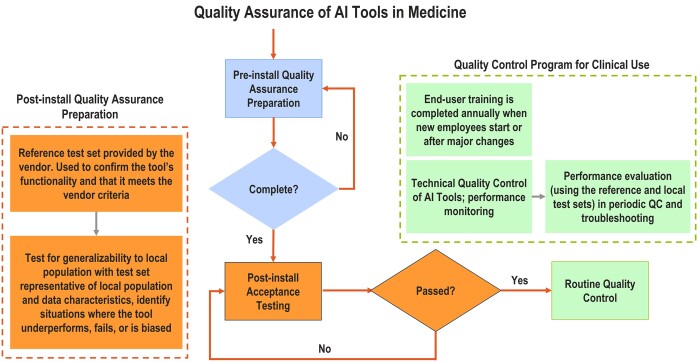
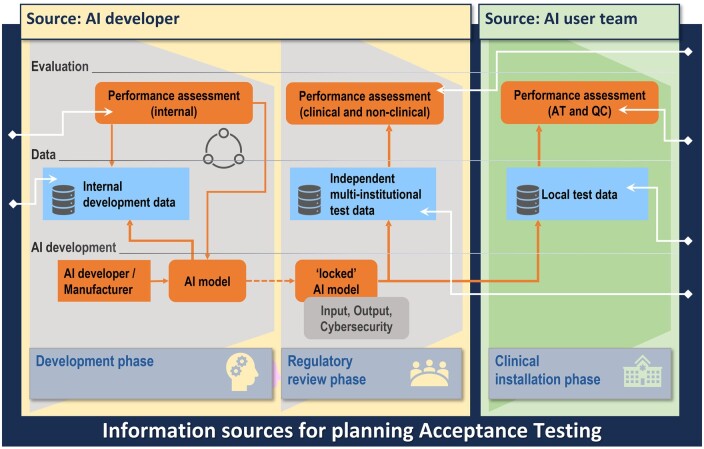
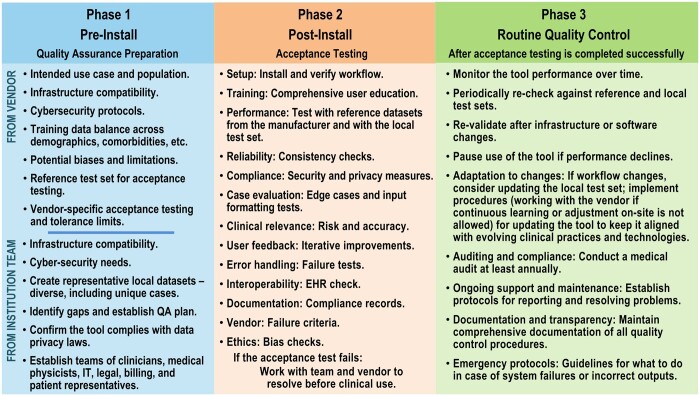
The adoption of artificial intelligence (AI) tools in medicine poses challenges to existing clinical workflows. This commentary discusses the necessity of context-specific quality assurance (QA), emphasizing the need for robust QA measures with quality control (QC) procedures that encompass (1) acceptance testing (AT) before clinical use, (2) continuous QC monitoring, and (3) adequate user training. The discussion also covers essential components of AT and QA, illustrated with real-world examples. We also highlight what we see as the shared responsibility of manufacturers or vendors, regulators, healthcare systems, medical physicists, and clinicians to enact appropriate testing and oversight to ensure a safe and equitable transformation of medicine through AI.
Keywords: acceptance testing; artificial intelligence; deep learning; machine learning; quality assurance; quality control; radiology.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Institute of Radiology.
Conflict of interest statement
U.M., A.S.-D., H.-P.C., R.K.S., D.V., H.G., N.P., B.S., Z.H., K.C., G.T., T.M.D., D.R., R.M., and L.H. have nothing to disclose. K.D. receives royalties from Hologic. Q.C. has received compensations from Carina Medical LLC, not related to this work, provides consulting services for Reflexion Medical, not related to this work. R.M.S. received royalties for patents or software licenses from iCAD, Philips, ScanMed, Translation Holdings, PingAn, and MGB, and received research support from PingAn through a Cooperative Research and Development Agreement, not related to this work. J.J.N. has received royalties from Hologic and from MEDIAN Technologies, through the University of Chicago licensing, not related to this work. H.Y. has received royalties from licensing fees to Hologic and Medians Technologies through the University of Chicago licensing, not related to this work. K.S. provides consulting services for Canon Medical, not related to this work. L.M. has received funding from HealthTriagesrl, not related to this work. H.H. has received funding from Siemens Healthineers for a scientific research project, not related to this work. SG.A. III has received royalties and licensing fees for computer-aided diagnosis through the University of Chicago Consultant, Novartis, not related to this work.
Figures
Similar articles
-
TU-E-218-01: PET/CT QA/QC and Acceptance Testing.Med Phys. 2012 Jun;39(6Part24):3916-3917. doi: 10.1118/1.4735985. Med Phys. 2012. PMID: 28518678
-
Mapping the Landscape of Care Providers' Quality Assurance Approaches for AI in Diagnostic Imaging.J Digit Imaging. 2023 Apr;36(2):379-387. doi: 10.1007/s10278-022-00731-7. Epub 2022 Nov 9. J Digit Imaging. 2023. PMID: 36352164 Free PMC article. Review.
-
Fairness of artificial intelligence in healthcare: review and recommendations.Jpn J Radiol. 2024 Jan;42(1):3-15. doi: 10.1007/s11604-023-01474-3. Epub 2023 Aug 4. Jpn J Radiol. 2024. PMID: 37540463 Free PMC article. Review.
-
Radiographic quality control devices.Health Devices. 2000 Apr;29(4):97-139. Health Devices. 2000. PMID: 11002439
-
Cybersecurity considerations for radiology departments involved with artificial intelligence.Eur Radiol. 2023 Dec;33(12):8833-8841. doi: 10.1007/s00330-023-09860-1. Epub 2023 Jul 7. Eur Radiol. 2023. PMID: 37418025 Free PMC article. Review.
Cited by
-
The artificial intelligence revolution in gastric cancer management: clinical applications.Cancer Cell Int. 2025 Mar 21;25(1):111. doi: 10.1186/s12935-025-03756-4. Cancer Cell Int. 2025. PMID: 40119433 Free PMC article. Review.
-
Advances in personalized medicine: translating genomic insights into targeted therapies for cancer treatment.Ann Transl Med. 2025 Apr 30;13(2):18. doi: 10.21037/atm-25-34. Epub 2025 Apr 29. Ann Transl Med. 2025. PMID: 40438512 Free PMC article. Review.
-
Artificial Intelligence in the Management of Malnutrition in Cancer Patients: A Systematic Review.Adv Nutr. 2025 Jul;16(7):100438. doi: 10.1016/j.advnut.2025.100438. Epub 2025 May 5. Adv Nutr. 2025. PMID: 40334987 Free PMC article. Review.
-
Bridging the gap: Phage manufacturing processes from laboratory to agri-food industry.Virus Res. 2025 Mar;353:199537. doi: 10.1016/j.virusres.2025.199537. Epub 2025 Jan 31. Virus Res. 2025. PMID: 39880310 Free PMC article. Review.
-
Quantitative image quality metrics enable resource-efficient quality control of clinically applied AI-based reconstructions in MRI.MAGMA. 2025 Jul;38(3):547-560. doi: 10.1007/s10334-025-01253-3. Epub 2025 May 24. MAGMA. 2025. PMID: 40411676 Free PMC article.
References
-
- Davis MA, Lim N, Jordan J, Yee J, Gichoya JW, Lee R.. Imaging artificial intelligence: a framework for radiologists to address health equity, from the AJR special series on DEI. AJR. 2023;221(3):302-308. - PubMed
-
- Geis JR, Brady AP, Wu CC, et al.Ethics of artificial intelligence in radiology: summary of the joint European and North American multisociety statement. Radiology. 2019;293(2):436-440. - PubMed
-
- Mezrich JL. Is artificial intelligence (AI) a pipe dream? Why legal issues present significant hurdles to AI autonomy. AJR Am J Roentgenol. 2022;219(1):152-156. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources