

Efficacy and safety of atezolizumab plus bevacizumab in patients with portal hypertension for unresectable hepatocellular carcinoma
- PMID: 38477514
- PMCID: PMC10935873
- DOI: 10.1002/cam4.7025
Efficacy and safety of atezolizumab plus bevacizumab in patients with portal hypertension for unresectable hepatocellular carcinoma
Abstract
Aim: Atezolizumab plus bevacizumab combination therapy (Atezo + Beva) is used as the first-line therapy for unresectable hepatocellular carcinoma (u-HCC). Serious adverse events (AEs), including rupture of esophagogastric varices, have been seen during treatment. Therefore, the relationships of efficacy, safety, and portal hypertension (PH) were analyzed.
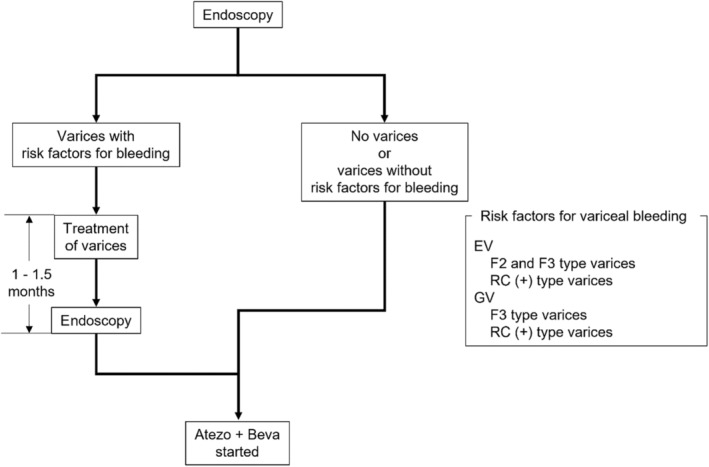
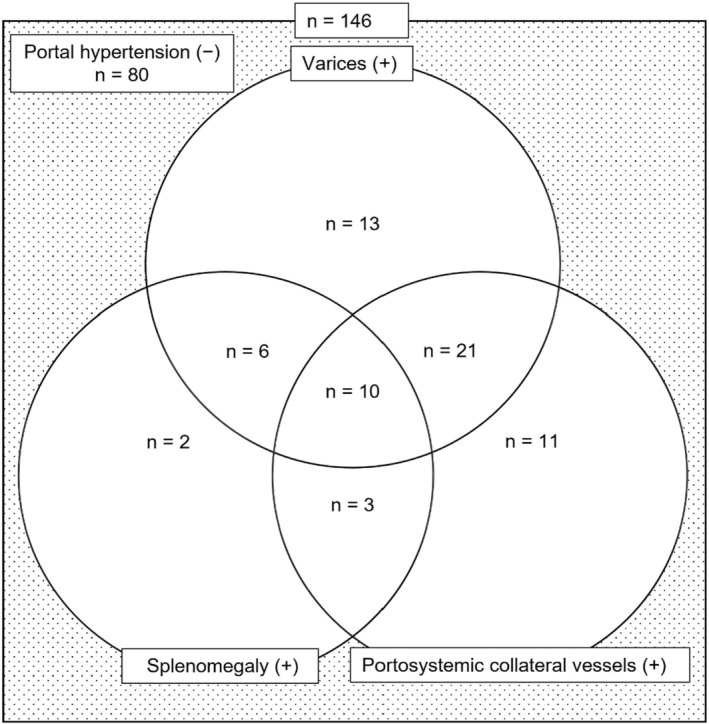
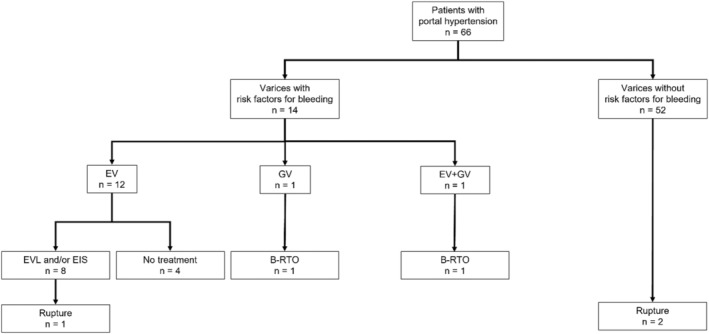
Methods: A total of 146 patients with u-HCC and Child-Pugh Scores of 5-7 received Atezo + Beva. Prophylactic treatment for varices was performed for patients with the risk of rupture of varices before the start of Atezo + Beva. A propensity score-matched cohort was created to minimize the risk of potential confounders. Efficacy was assessed in 41 propensity score-matched pairs. AEs were assessed between patients without PH (n = 80) and with PH (n = 66).
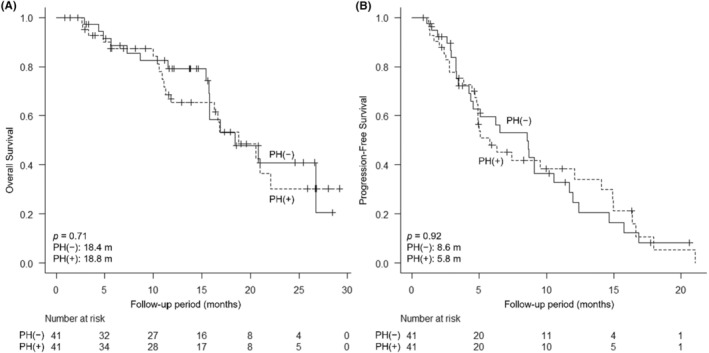
Results: In patients without PH and with PH, median overall survival was 18.4 months and 18.8 months (p = 0.71), and median progression-free survival was 8.6 months and 5.8 months (p = 0.92), respectively. On the best radiological response evaluation for Response Evaluation Criteria in Solid Tumors, the objective response rate was 31.7% and 26.8% (p = 0.81), respectively. Variceal rupture occurred in three patients with PH, but there were no significant differences in the occurrence of variceal rupture (p = 0.090) and Grade 3-4 AEs between patients without and with PH.
Conclusions: No significant differences in efficacy and safety were observed with PH. Prophylactic treatment for varices before the start of Atezo + Beva would allow treatment to continue relatively safely.
Keywords: adverse events; atezolizumab plus bevacizumab; esophagogastric variceal rupture; hepatocellular carcinoma; portal hypertension.
© 2024 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Authors declare no conflict of interests for this article.
Figures
Similar articles
-
Comparison of Efficacy and Safety of Atezolizumab Plus Bevacizumab and Lenvatinib as First-Line Therapy for Unresectable Hepatocellular Carcinoma: A Propensity Score Matching Analysis.Target Oncol. 2022 Nov;17(6):643-653. doi: 10.1007/s11523-022-00921-x. Epub 2022 Oct 22. Target Oncol. 2022. PMID: 36272060 Free PMC article.
-
Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): an open-label, multicentre, phase 1b study.Lancet Oncol. 2020 Jun;21(6):808-820. doi: 10.1016/S1470-2045(20)30156-X. Lancet Oncol. 2020. PMID: 32502443 Clinical Trial.
-
Tiragolumab in combination with atezolizumab and bevacizumab in patients with unresectable, locally advanced or metastatic hepatocellular carcinoma (MORPHEUS-Liver): a randomised, open-label, phase 1b-2, study.Lancet Oncol. 2025 Feb;26(2):214-226. doi: 10.1016/S1470-2045(24)00679-X. Epub 2025 Jan 21. Lancet Oncol. 2025. PMID: 39855251 Clinical Trial.
-
Progression of portal hypertension after atezolizumab plus bevacizumab for hepatocellular carcinoma-report a case and literature review.J Formos Med Assoc. 2024 Aug;123(8):916-919. doi: 10.1016/j.jfma.2024.03.019. Epub 2024 Apr 2. J Formos Med Assoc. 2024. PMID: 38565487 Review.
-
Prognosis and treatment pattern of advanced hepatocellular carcinoma after failure of first-line atezolizumab and bevacizumab treatment.Hepatol Int. 2022 Oct;16(5):1199-1207. doi: 10.1007/s12072-022-10392-x. Epub 2022 Aug 20. Hepatol Int. 2022. PMID: 35986846 Review.
Cited by
-
Role of Vascular Liver Diseases in Hepatocellular Carcinoma Development.Cancers (Basel). 2025 Jun 20;17(13):2060. doi: 10.3390/cancers17132060. Cancers (Basel). 2025. PMID: 40647361 Free PMC article. Review.
-
Partial Splenic Embolization for Portal Hypertension Exacerbation During Atezolizumab/Bevacizumab Combination Therapy in Unresectable Hepatocellular Carcinoma.In Vivo. 2025 Mar-Apr;39(2):936-941. doi: 10.21873/invivo.13898. In Vivo. 2025. PMID: 40010973 Free PMC article.
-
The current status and future of targeted-immune combination for hepatocellular carcinoma.Front Immunol. 2024 Aug 5;15:1418965. doi: 10.3389/fimmu.2024.1418965. eCollection 2024. Front Immunol. 2024. PMID: 39161764 Free PMC article. Review.
References
-
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391:1301‐1314. - PubMed
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69‐90. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378‐390. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
