

Safety and efficacy of dynamic catheter-directed cerebral digital subtraction angiography for diagnosis of bowhunter syndrome spectrum disorders: A systematic review of the literature
- PMID: 38477583
- PMCID: PMC11577335
- DOI: 10.1177/15910199241236820
Safety and efficacy of dynamic catheter-directed cerebral digital subtraction angiography for diagnosis of bowhunter syndrome spectrum disorders: A systematic review of the literature
Abstract
Introduction: Dynamic catheter-directed cerebral digital subtraction angiography (dcDSA) is the gold standard for diagnosing dynamic vascular occlusion syndromes such as bowhunter syndrome (BHS). Nonetheless, concerns about its safety exist and no standardized protocols have been published to date.
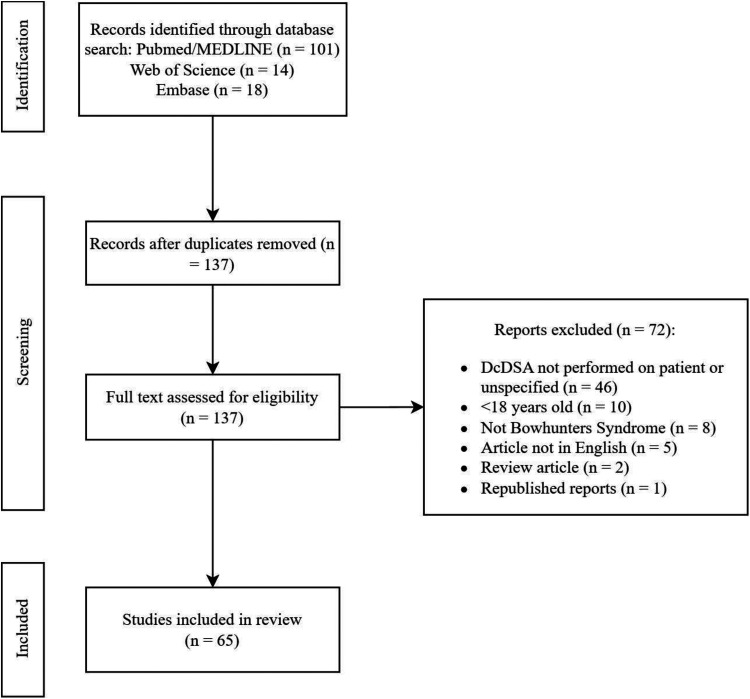
Methods: We describe our methodology and insights regarding the use of dcDSA in patients with BHS. We also perform a systematic literature review to identify cases of typical and atypical presentations of BHS wherein dcDSA was utilized and report on any procedural complications related to dcDSA.
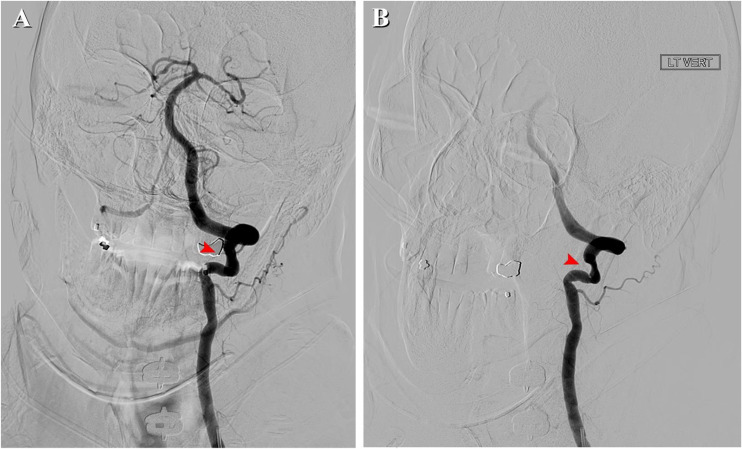
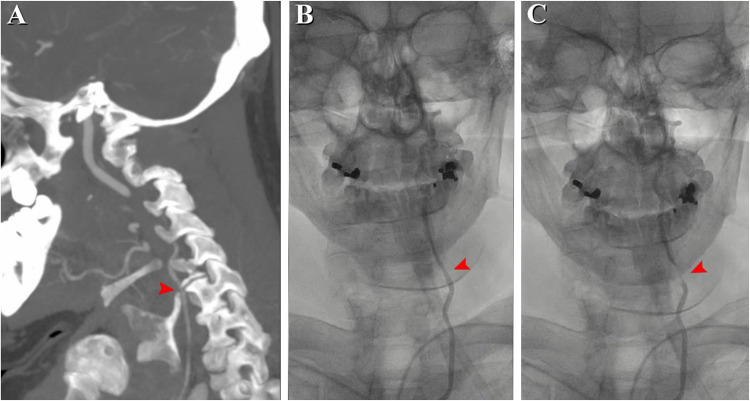
Results: Our study included 104 cases wherein dcDSA was used for the diagnosis of BHS. There were 0 reported complications of dcDSA. DcDSA successfully established diagnosis in 102 of these cases. Thirty-eight cases were deemed atypical presentations of BHS. Fourteen patients endorsed symptoms during neck flexion/extension. In eight cases, there was dynamic occlusion of bilateral vertebral arteries during a single maneuver. Three patients had multiple areas of occlusion along a single vertebral artery (VA). An anomalous entry of the VA above the C6 transverse foramen was observed in four patients. One patient had VA occlusion with neutral head position and recanalization upon contralateral lateral head tilt.
Conclusion: Our study highlights the safety and diagnostic benefits of dcDSA in characterizing the broad spectrum of BHS pathology encountered in clinical practice. This technique offers a powerful means to evaluate changes in cerebral blood flow and cervical arterial morphology in real time, overcoming the constraints of static imaging methods. Our findings pave the way for further studies on dcDSA to enhance cross-sectional imaging methods for the characterization of BHS and other dynamic vascular occlusion syndromes.
Keywords: Cerebral digital subtraction angiography; bowhunter syndrome; dynamic vascular occlusion syndrome.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Shaban S, Huasen B, Haridas A, et al. Digital subtraction angiography in cerebrovascular disease: current practice and perspectives on diagnosis, acute treatment and prognosis. Acta Neurol Belg 2022; 122: 763–780. - PubMed
-
- Baranoski JF, White AC, Chung CY, et al. Mechanical disorders of the cervicocerebral circulation in children and young adults. J NeuroIntervent Surg. 2023: 1–8. - PubMed
-
- Sorensen BF. Bow hunter’s stroke. Neurosurgery 1978; 2: 259–261. - PubMed
-
- Jongbloed W, Gertel A, Kashat L, et al. Vertebral artery compression by the greater cornu of the thyroid cartilage. Ear Nose Throat J 2023; 102: 301–303. - PubMed
-
- Rollins N, Booth T, Shapiro K. The use of gated cine phase contrast and MR venography in achondroplasia. Childs Nerv Syst 2000; 16: 569–575. discussion 575–577. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
