

Chest tube removal at different gas flows in prolonged air leak: a randomized non-inferiority trial
- PMID: 38479816
- PMCID: PMC10963076
- DOI: 10.1093/ejcts/ezae097
Chest tube removal at different gas flows in prolonged air leak: a randomized non-inferiority trial
Abstract
Objectives: To evaluate the safety and feasibility of removing drainage tubes at larger size of air leak in patients with prolonged air leak after pulmonary surgery.
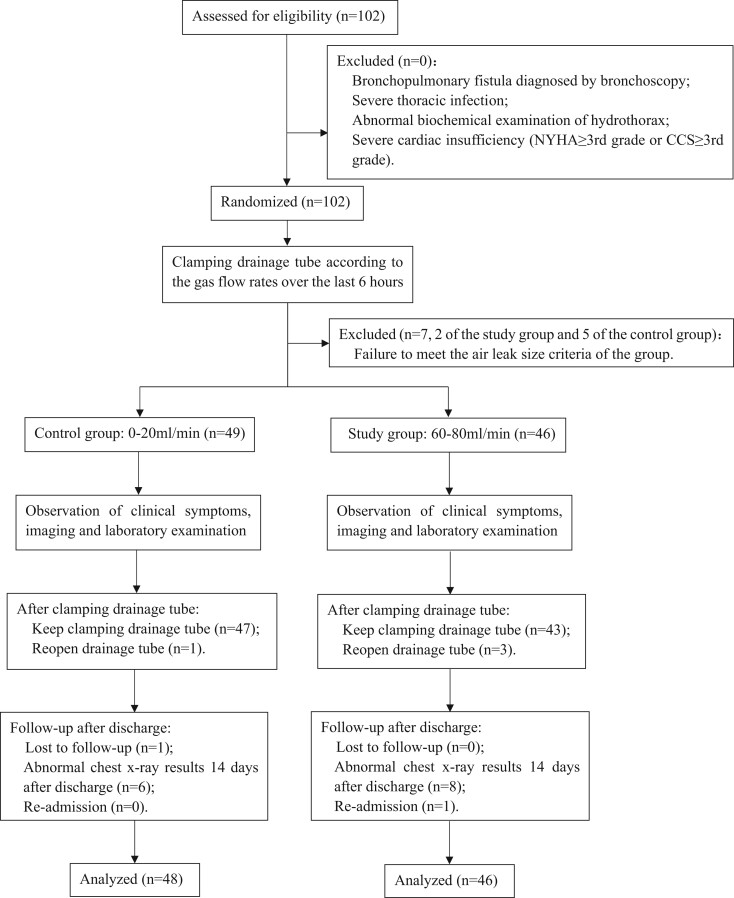
Methods: Ninety-five patients who underwent pulmonary surgery with prolonged air leak in our centre were enrolled in this randomized controlled, single-centre, non-inferiority study. The drainage tube was clamped with a stable size of air leak observed over the last 6 h, which was quantified by gas flow rate using the digital drainage system. The control group (n = 48) and the study group (n = 46) had their drainage tube clamped at 0-20 ml/min and 60-80 ml/min, respectively. We continuously monitored clinical symptoms, conducted imaging and laboratory examinations, and decided whether to reopen the drainage tube.
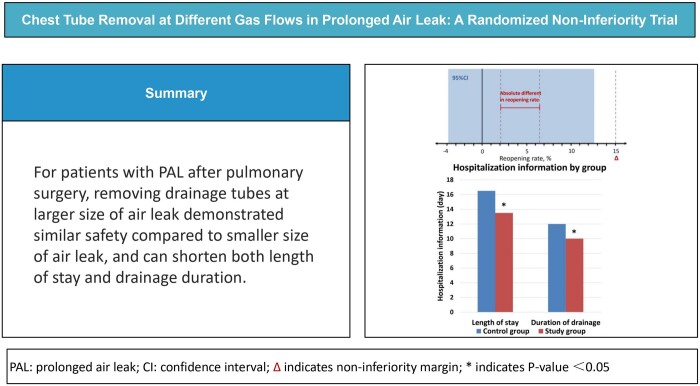
Results: The reopening rate in the study group was not lower than that in the control group (2.08% vs 6.52%, P > 0.05). The absolute difference in reopening rate was 4.44% (95% confidence interval -0.038 to 0.126), with an upper limit of 12.6% below the non-inferiority margin (15%). There were significant differences in the length of stay [16.5 (13-24.75) vs 13.5 (12-19.25), P = 0.017] and the duration of drainage [12 (9.25-18.50) vs 10 (8-12.25), P = 0.007] between the control and study groups. No notable differences were observed in chest X-ray results 14 days after discharge or in the readmission rate.
Conclusions: For patients with prolonged air leak, removing drainage tubes at larger size of air leak demonstrated similar safety compared to smaller size of air leak, and can shorten both length of stay and drainage duration.
Clinical trial registration number: Name of registry: Gas flow threshold for safe removal of chest drainage in patients with alveolar-pleural fistula prolonged air leak after pulmonary surgery. Registration number: ChiCTR2200067120. URL: https://www.chictr.org.cn/.
Keywords: Chest drainage tube removal; Digital drainage system; Intrapleural pressure; Prolonged air leak; Pulmonary surgery.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
Comment in
-
Chest tube management in lung surgery: 'no bubbles-no troubles' is not always true.Eur J Cardiothorac Surg. 2024 May 3;65(5):ezae186. doi: 10.1093/ejcts/ezae186. Eur J Cardiothorac Surg. 2024. PMID: 38704862 No abstract available.
-
Advanced digital monitoring: is it a replacement for current chest tube removal methods?Eur J Cardiothorac Surg. 2024 Jul 1;66(1):ezae287. doi: 10.1093/ejcts/ezae287. Eur J Cardiothorac Surg. 2024. PMID: 39047156 No abstract available.
References
-
- Singhal S, Ferraris VA, Bridges CR, Clough ER, Mitchell JD, Fernando HC. et al. Management of alveolar air leaks after pulmonary resection. Ann Thorac Surg 2010;89:1327–35. - PubMed
-
- Suzuki K, Saji H, Aokage K, Watanabe S-I, Okada M, Mizusawa J. et al.; Japan Clinical Oncology Group. Comparison of pulmonary segmentectomy and lobectomy: safety results of a randomized trial. J Thorac Cardiovasc Surg 2019;158:895–907. - PubMed
