

Characteristics of pulse oximetry and arterial blood gas in patients with fibrotic interstitial lung disease
- PMID: 38479819
- PMCID: PMC10941153
- DOI: 10.1136/bmjresp-2023-002250
Characteristics of pulse oximetry and arterial blood gas in patients with fibrotic interstitial lung disease
Abstract
Background: Fibrotic interstitial lung disease (ILD) is frequently associated with abnormal oxygenation; however, little is known about the accuracy of oxygen saturation by pulse oximetry (SpO2) compared with arterial blood gas (ABG) saturation (SaO2), the factors that influence the partial pressure of carbon dioxide (PaCO2) and the impact of PaCO2 on outcomes in patients with fibrotic ILD.
Study design and methods: Patients with fibrotic ILD enrolled in a large prospective registry with a room air ABG were included. Prespecified analyses included testing the correlation between SaO2 and SpO2, the difference between SaO2 and SpO2, the association of baseline characteristics with both the difference between SaO2 and SpO2 and the PaCO2, the association of baseline characteristics with acid-base category, and the association of PaCO2 and acid-base category with time to death or transplant.
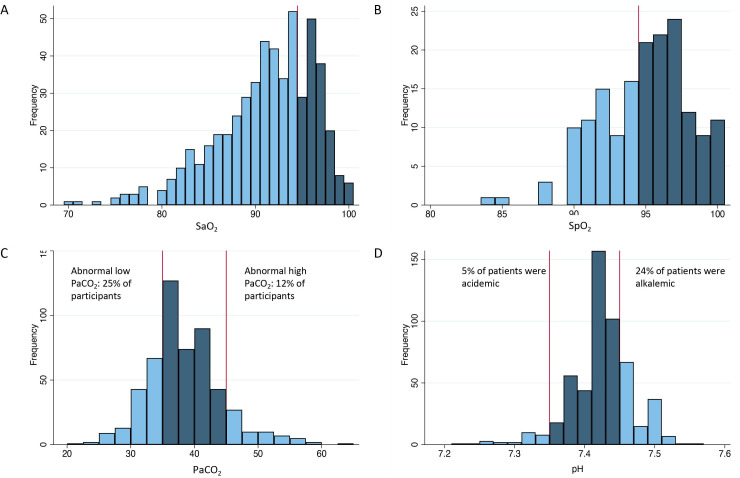
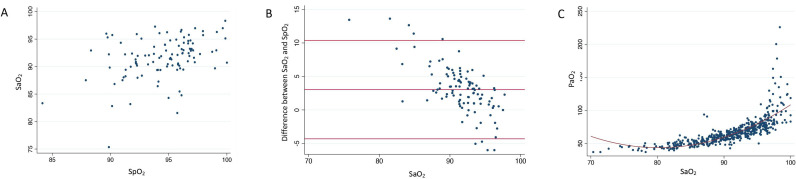
Results: A total of 532 patients with fibrotic ILD were included. Mean resting SaO2 was 92±4% and SpO2 was 95±3%. Mean PaCO2 was 38±6 mmHg, with 135 patients having PaCO2 <35 mmHg and 62 having PaCO2 >45 mmHg. Correlation between SaO2 and SpO2 was mild to moderate (r=0.39), with SpO2 on average 3.0% higher than SaO2. No baseline characteristics were associated with the difference in SaO2 and SpO2. Variables associated with either elevated or abnormal (elevated or low) PaCO2 included higher smoking pack-years and lower baseline forced vital capacity (FVC). Lower baseline lung function was associated with an increased risk of chronic respiratory acidosis. PaCO2 and acid-base status were not associated with time to death or transplant.
Interpretation: SaO2 and SpO2 are weakly-to-moderately correlated in fibrotic ILD, with limited ability to accurately predict this difference. Abnormal PaCO2 was associated with baseline FVC but was not associated with outcomes.
Keywords: interstitial fibrosis.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MAD reports no conflicts of interest relevant to this manuscript. KD reports no conflicts of interest relevant to this manuscript. DA reports grants and personal fees from Boehringer Ingelheim, grants from Canadian Institute for Health Research and from Fonds de Recherche du Quebec en Santé. CD reports no conflicts of interest relevant to this manuscript. JHF reports personal fees from AstraZeneca and Boehringer Ingelheim. KJ reports grants from Boehringer Ingelheim, Pulmonary Fibrosis Society of Calgary, University of Calgary School of Medicine; personal fees from Boehringer Ingelheim, Roche, Three Lakes Foundation, Pliant Therapeutics, Theravance, Blade Therapeutics. MK reports grants from Canadian Institute for Health Research, Roche, Boehringer Ingelheim, Pieris, Prometic; personal fees from Boehringer Ingelheim, Roche, European Respiratory Journal, Belerophon, United Therapeutics, Nitto Denko, MitoImmune, Pieris, AbbVie, DevPro Biopharma, Horizon, Algernon, CSL Behring. SDL reports consulting/personal fees and moderator honoraria from Boehringer-Ingelheim, honoraria from Hoffman-La Roche Ltd, grants from AstraZeneca and the University of Saskatchewan. HM reports grants from Boehringer Ingelheim and Gilead. VM reports grants from Boehringer Ingelheim, AstraZeneca, and Roche; personal fees from Boehringer Ingelheim and Roche. BM reports no conflicts of interest relevant to this manuscript. JM reports personal fees from Boehringer Ingelheim and Roche. D-CM reports personal fees from Boehringer Ingelheim. CJR reports grants from Boehringer Ingelheim; personal fees from AstraZeneca, Boehringer Ingelheim, Roche, Pliant Therapeutics, Cipla, Veracyte.
Figures

Similar articles
-
Comparative Analysis of Oxygen Saturation by Pulse Oximetry and Arterial Blood Gas in Hypoxemic Patients in a Tertiary Care Hospital.Cureus. 2023 Jul 25;15(7):e42447. doi: 10.7759/cureus.42447. eCollection 2023 Jul. Cureus. 2023. PMID: 37637606 Free PMC article.
-
Facing SpO2 and SaO2 discrepancies in ICU patients: is the perfusion index helpful?J Clin Monit Comput. 2020 Aug;34(4):693-698. doi: 10.1007/s10877-019-00371-3. Epub 2019 Aug 7. J Clin Monit Comput. 2020. PMID: 31392655 Free PMC article.
-
Pulse Oximetry and Arterial Oxygen Saturation during Cardiopulmonary Exercise Testing.Med Sci Sports Exerc. 2018 Oct;50(10):1992-1997. doi: 10.1249/MSS.0000000000001658. Med Sci Sports Exerc. 2018. PMID: 29771822 Free PMC article.
-
[Feasibility of pulse oxygen saturation for the condition evaluation of acute respiratory distress syndrome patients in the Lijiang region].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Dec;33(12):1447-1452. doi: 10.3760/cma.j.cn121430-20210518-00737. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 35131011 Chinese.
-
Pulse oximetry: fundamentals and technology update.Med Devices (Auckl). 2014 Jul 8;7:231-9. doi: 10.2147/MDER.S47319. eCollection 2014. Med Devices (Auckl). 2014. PMID: 25031547 Free PMC article. Review.
References
-
- Ebmeier SJ, Barker M, Bacon M, et al. . Accuracy of pulse oximetry recordings in ICU patients: A two centre observational study of simultaneous pulse oximetry and arterial oxygen saturation recordings in intensive care unit patients. Anaesth Intensive Care 2018;46:297–303. 10.1177/0310057X1804600307 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical