

Salvage endoscopic nasopharyngectomy for recurrent nasopharyngeal carcinoma in a non-endemic area
- PMID: 38480535
- PMCID: PMC11211200
- DOI: 10.1007/s00405-024-08500-8
Salvage endoscopic nasopharyngectomy for recurrent nasopharyngeal carcinoma in a non-endemic area
Abstract
Purpose: To analyze oncological outcomes of endoscopic surgical treatment of locally recurrent EBV-related undifferentiated non-keratinizing nasopharyngeal carcinoma (uNK-NPC) in a non-endemic area.
Methods: Retrospective review of patients affected by recurrent uNK-NPC treated with nasopharyngeal endoscopic resection (NER) in a tertiary-care referral center from 2003 to 2022, by evaluating survival rates, prognostic factors, and follow-up strategies.
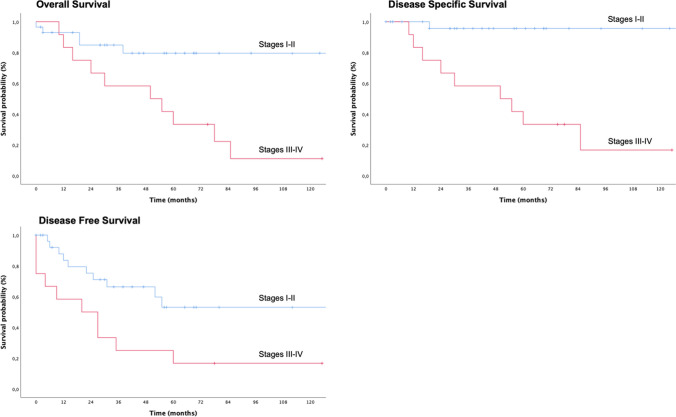
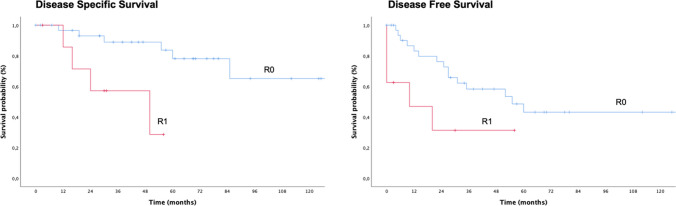
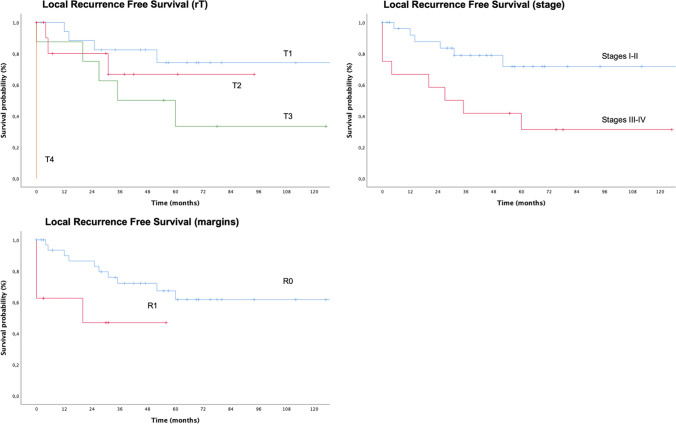
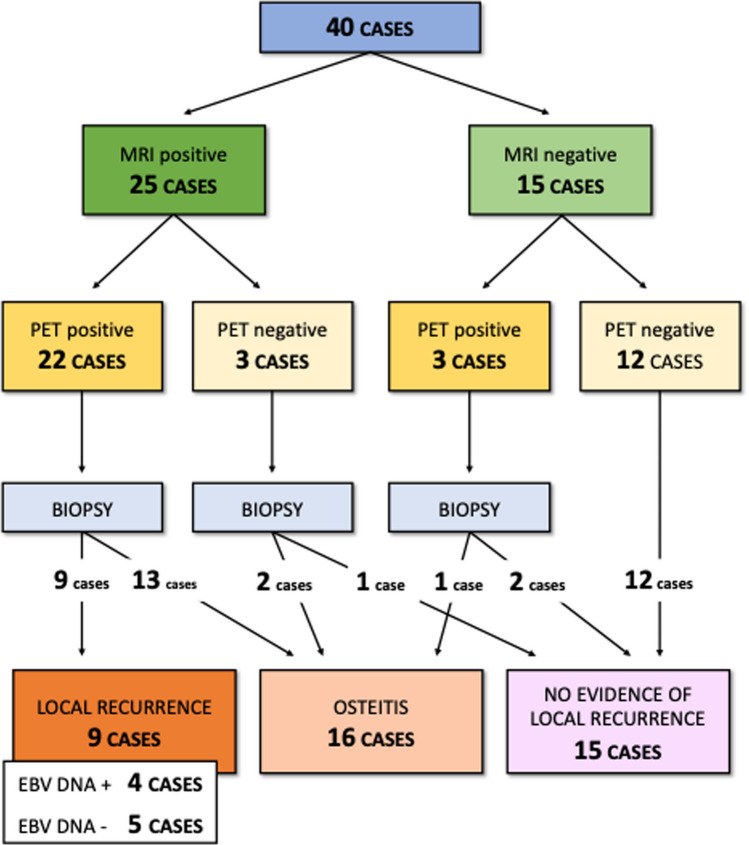
Results: The oncological outcomes of 41 patients were analyzed, over a mean follow-up period of 57 months. The 5-year overall, disease-specific, and disease-free survival of the cohort were 60.7% ± 8.9%, 69% ± 9%, and 39.7% ± 9.2%, respectively. The local (rT) and regional (rN) extension of recurrent disease, stage of disease, and status of resection margins appeared to significantly influence survivals. After a mean follow-up period of 21 months, a further recurrence after NER was observed in 36.6% of cases. Skull base osteonecrosis induced by previous irradiation and post-surgical bone remodeling represent the major challenges for early detection of further local relapses during postoperative follow-up.
Conclusion: NER appeared as a safe and effective treatment for recurrent uNK-NPC. The adequate selection of patients eligible for NER is essential, to maximize the chances to cure and minimize the risk of local complications.
Keywords: EBV; Endoscopic nasopharyngectomy; Head and neck oncology; Nasopharyngeal carcinoma; Skull base.
© 2024. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Targeted endoscopic salvage nasopharyngectomy for recurrent nasopharyngeal carcinoma.Int Forum Allergy Rhinol. 2012 Mar-Apr;2(2):166-73. doi: 10.1002/alr.20111. Epub 2011 Dec 13. Int Forum Allergy Rhinol. 2012. PMID: 22170783
-
5-year outcomes of salvage endoscopic nasopharyngectomy for recurrent nasopharyngeal carcinoma.J Otolaryngol Head Neck Surg. 2021 Feb 17;50(1):12. doi: 10.1186/s40463-020-00482-x. J Otolaryngol Head Neck Surg. 2021. PMID: 33597031 Free PMC article.
-
A 4-year review of surgical and oncological outcomes of endoscopic endonasal transpterygoid nasopharyngectomy in salvaging locally recurrent nasopharyngeal carcinoma.Eur Arch Otorhinolaryngol. 2019 Sep;276(9):2475-2482. doi: 10.1007/s00405-019-05522-5. Epub 2019 Jun 21. Eur Arch Otorhinolaryngol. 2019. PMID: 31227870
-
Salvage surgery in nasopharyngeal Cancer: Unraveling the efficacy of transnasal endoscopic nasopharyngectomy for advanced stage recurrent tumors.Oral Oncol. 2024 Dec;159:107048. doi: 10.1016/j.oraloncology.2024.107048. Epub 2024 Oct 2. Oral Oncol. 2024. PMID: 39362026
-
Endoscopic nasopharyngectomy and its role in managing locally recurrent nasopharyngeal carcinoma.Otolaryngol Clin North Am. 2011 Oct;44(5):1141-54. doi: 10.1016/j.otc.2011.07.002. Otolaryngol Clin North Am. 2011. PMID: 21978898 Review.
Cited by
-
Margins in oncologic nasopharyngeal surgery: a systematic review with meta-analysis.Acta Otorhinolaryngol Ital. 2025 May;45(Suppl. 1):S56-S70. doi: 10.14639/0392-100X-suppl.1-45-2025-N1170. Acta Otorhinolaryngol Ital. 2025. PMID: 40400377 Free PMC article.
-
Endoscopic-Assisted Transoral Approach (EATA) for Extracranial Tumors: A Multicentric Case Series.Life (Basel). 2025 Jun 18;15(6):975. doi: 10.3390/life15060975. Life (Basel). 2025. PMID: 40566631 Free PMC article.
-
Key Risk Factors for Postoperative Hypotension in Nasopharyngeal Carcinoma Patients After Endoscopic Surgery: A Retrospective Study.Med Sci Monit. 2025 Jun 8;31:e948124. doi: 10.12659/MSM.948124. Med Sci Monit. 2025. PMID: 40483555 Free PMC article.
References
-
- El-Naggar AK, Chan JKC, Grandis JR, Takashi Takata PJS (2017) World health organization classification of head and neck tumors – International Agency fo Research on Cancer (IARC) – 4th Edition
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
