

Is Robotic Surgery the Future for Resectable Esophageal Cancer?: A Systematic Literature Review of Oncological and Clinical Outcomes
- PMID: 38480565
- PMCID: PMC11164768
- DOI: 10.1245/s10434-024-15148-5
Is Robotic Surgery the Future for Resectable Esophageal Cancer?: A Systematic Literature Review of Oncological and Clinical Outcomes
Abstract
Background: Radical esophagectomy for resectable esophageal cancer is a major surgical intervention, associated with considerable postoperative morbidity. The introduction of robotic surgical platforms in esophagectomy may enhance advantages of minimally invasive surgery enabled by laparoscopy and thoracoscopy, including reduced postoperative pain and pulmonary complications. This systematic review aims to assess the clinical and oncological benefits of robot-assisted esophagectomy.
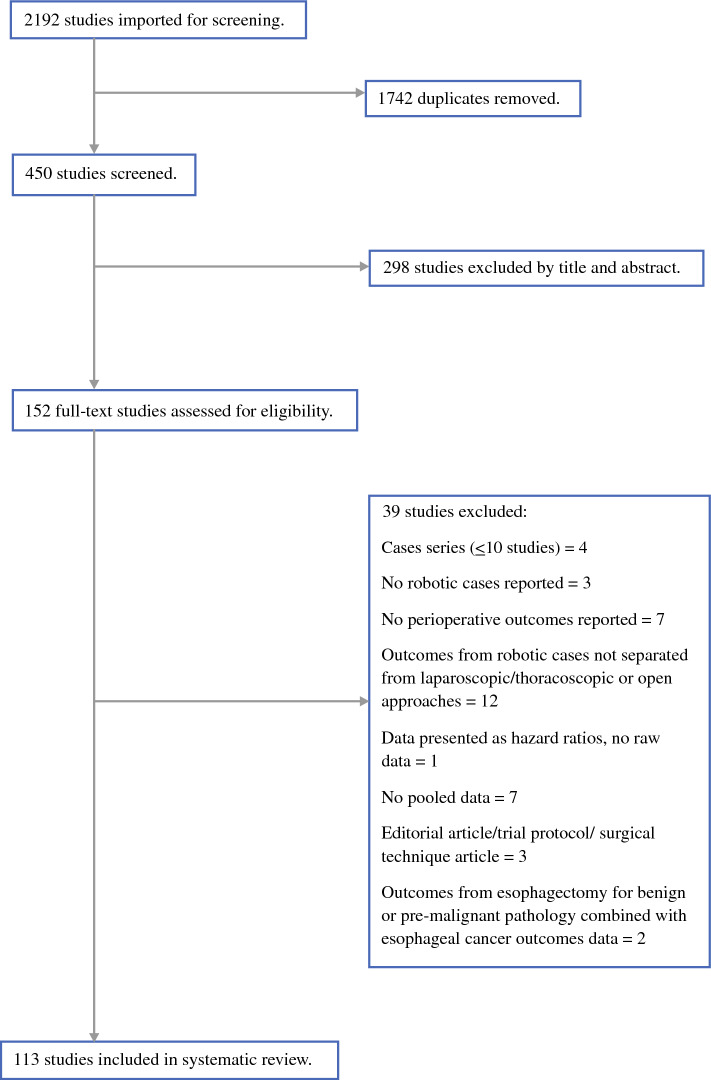
Methods: A systematic literature search of the MEDLINE (PubMed), Embase and Cochrane databases was performed for studies published up to 1 August 2023. This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocols and was registered in the PROSPERO database (CRD42022370983). Clinical and oncological outcomes data were extracted following full-text review of eligible studies.
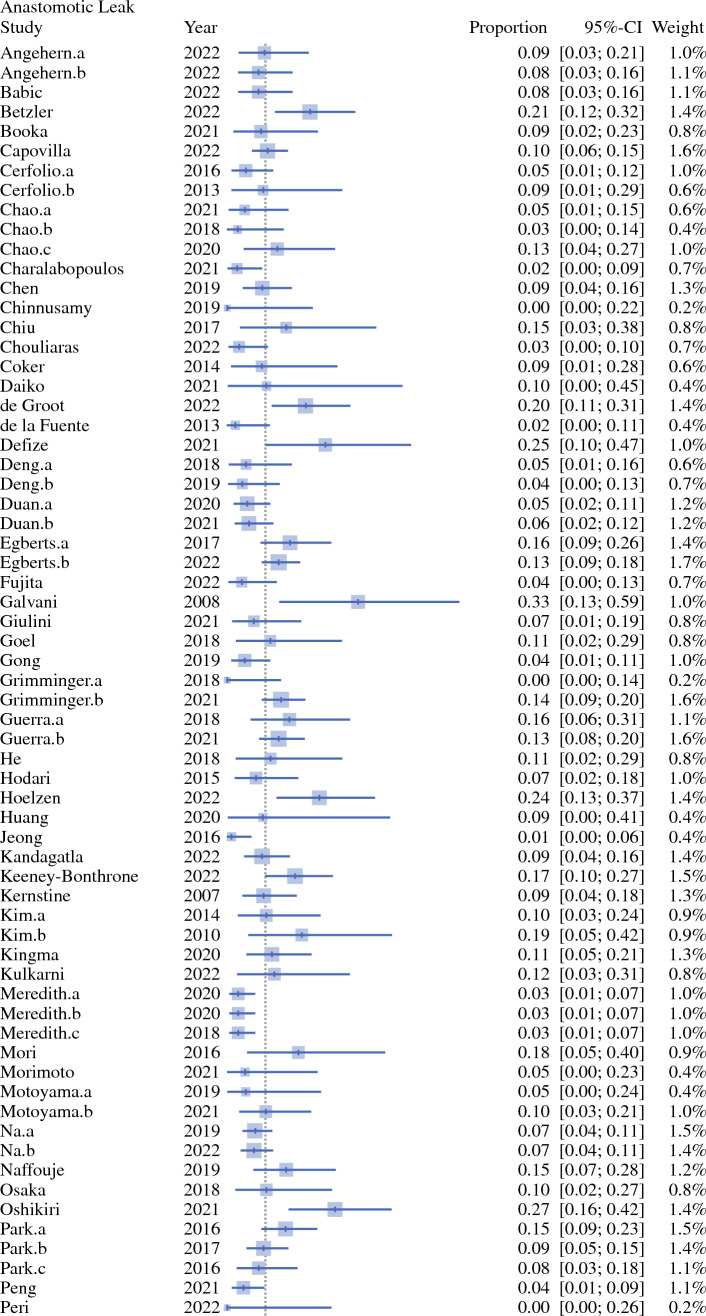
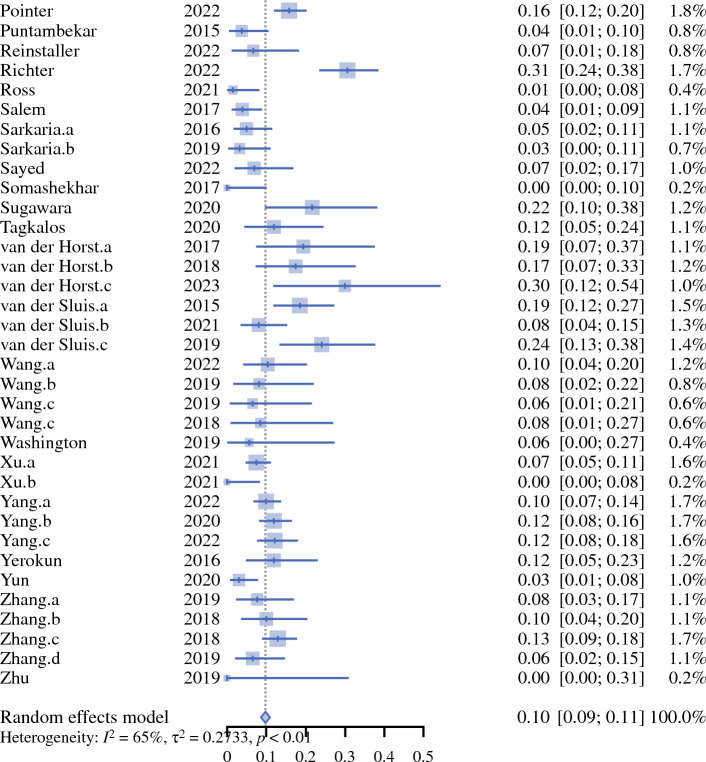
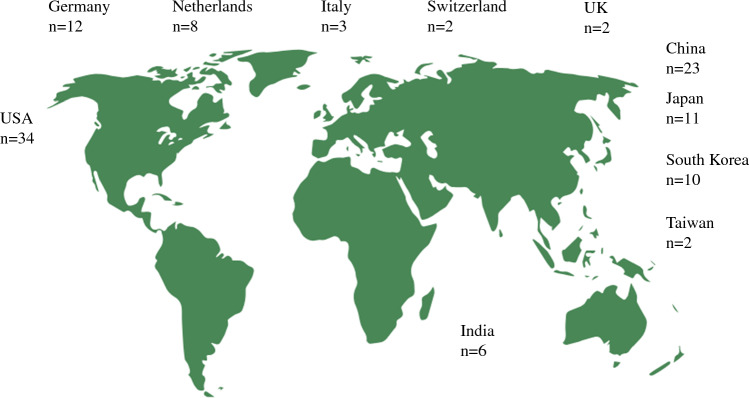
Results: A total of 113 studies (n = 14,701 patients, n = 2455 female) were included. The majority of the studies were retrospective in nature (n = 89, 79%), and cohort studies were the most common type of study design (n = 88, 79%). The median number of patients per study was 54. Sixty-three studies reported using a robotic surgical platform for both the abdominal and thoracic phases of the procedure. The weighted mean incidence of postoperative pneumonia was 11%, anastomotic leak 10%, total length of hospitalisation 15.2 days, and a resection margin clear of the tumour was achieved in 95% of cases.
Conclusions: There are numerous reported advantages of robot-assisted surgery for resectable esophageal cancer. A correlation between procedural volume and improvements in outcomes with robotic esophagectomy has also been identified. Multicentre comparative clinical studies are essential to identify the true objective benefit on outcomes compared with conventional surgical approaches before robotic surgery is accepted as standard of practice.
Keywords: Clinical outcomes; Esophageal cancer; Esophagectomy; Lymphadenectomy; Minimally invasive surgery; Oncological outcomes; Perioperative therapy; Robotic surgery.
© 2024. The Author(s).
Figures
Similar articles
-
Evaluating Postoperative Morbidity and Outcomes of Robotic-Assisted Esophagectomy in Esophageal Cancer Treatment-A Comprehensive Review on Behalf of TROGSS (The Robotic Global Surgical Society) and EFISDS (European Federation International Society for Digestive Surgery) Joint Working Group.Curr Oncol. 2025 Jan 28;32(2):72. doi: 10.3390/curroncol32020072. Curr Oncol. 2025. PMID: 39996872 Free PMC article. Review.
-
Short-term outcomes of robotic radical esophagectomy for esophageal cancer by a nontransthoracic approach compared with conventional transthoracic surgery.Dis Esophagus. 2016 Jul;29(5):429-34. doi: 10.1111/dote.12345. Epub 2015 Mar 23. Dis Esophagus. 2016. PMID: 25809390 Free PMC article.
-
Comparison of Clinical Outcomes of Robot-Assisted, Video-Assisted, and Open Esophagectomy for Esophageal Cancer: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2129228. doi: 10.1001/jamanetworkopen.2021.29228. JAMA Netw Open. 2021. PMID: 34724556 Free PMC article.
-
Robot-assisted transhiatal esophagectomy: a 3-year single-center experience.Dis Esophagus. 2013 Feb-Mar;26(2):159-66. doi: 10.1111/j.1442-2050.2012.01325.x. Epub 2012 Mar 6. Dis Esophagus. 2013. PMID: 22394116 Clinical Trial.
-
Robot-assisted esophagectomy (RAE) versus conventional minimally invasive esophagectomy (MIE) for resectable esophageal squamous cell carcinoma: protocol for a multicenter prospective randomized controlled trial (RAMIE trial, robot-assisted minimally invasive Esophagectomy).BMC Cancer. 2019 Jun 21;19(1):608. doi: 10.1186/s12885-019-5799-6. BMC Cancer. 2019. PMID: 31226960 Free PMC article. Clinical Trial.
Cited by
-
Digital health technologies in swallowing care from screening to rehabilitation: A narrative review.Auris Nasus Larynx. 2025 May 21;52(4):319-326. doi: 10.1016/j.anl.2025.05.002. Online ahead of print. Auris Nasus Larynx. 2025. PMID: 40403345 Review.
-
Short-and middle-term outcomes of robot-assisted minimally invasive esophagectomy for highly locally advanced esophageal cancer with stage cT3 borderline and cT4b at initial diagnosis.Surg Endosc. 2025 May;39(5):2994-3005. doi: 10.1007/s00464-025-11666-9. Epub 2025 Mar 21. Surg Endosc. 2025. PMID: 40116900
References
-
- van der Sluis PC, van der Horst S, May AM, et al. Robot-assisted minimally invasive thoracolaparoscopic esophagectomy versus open transthoracic esophagectomy for resectable esophageal cancer: a randomized controlled trial. Ann Surg. 2019;269(4):621–630. doi: 10.1097/SLA.0000000000003031. - DOI - PubMed
-
- Al-Batran S-E, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948–1957. doi: 10.1016/S0140-6736(18)32557-1. - DOI - PubMed
-
- Wang H, Tang H, Fang Y, et al. Morbidity and mortality of patients who underwent minimally invasive esophagectomy after neoadjuvant chemoradiotherapy vs neoadjuvant chemotherapy for locally advanced esophageal squamous cell carcinoma: a randomized clinical trial. JAMA Surg. 2021;156(5):444–451. doi: 10.1001/jamasurg.2021.0133. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
